1 | What embryologic structures give rise to the larynx? | The endodermal lining and splanchnic mesenchyme of the foregut formed by branchial arches IV through VI. |
2 | Match the branchial arch with its laryngeal derivative: A. Corniculate, arytenoid, and cricoid cartilages; some laryngeal muscles; recurrent laryngeal nerve B. Upper body of the hyoid bone and its lesser cornu C. Epiglottis, thyroid cartilage, cuneiform cartilages, pharyngeal constrictors, some laryngeal musculature, superior laryngeal nerve D. Lower body of the hyoid bone and its greater cornu | A. V/VI B. II C. IV D. III |
3 | The anlagen of the larynx, trachea, bronchia, and lungs arise from what embryologic structure? | The tracheobronchial groove, a ventromedial diverticulum of the foregut |
4 | What structure obliterates the ventral primitive laryngopharynx during embryologic development? | Epithelial lamina |
5 | In the postnatal period, the larynx undergoes changes in axis, shape, length, and position. Describe the position of the larynx related to the cervical vertebra in an infant versus an adult. | • Infant: C1–C4 • Adult (by age 6 years): C4–C7 |
6 | What are the nine laryngeal cartilages? | Unpaired 1: Cricoid cartilage 2: Thyroid cartilage 3: Epiglottis Paired 4,5: Arytenoid cartilages 6,7: Corniculate cartilages 8,9: Cuneiform cartilages |
7 | Name the six intrinsic muscles of the larynx, and describe both their function and innervation. ( | • Cricothyroid: Lengthens the vocal cord; external branch of the superior laryngeal nerve (cranial nerve [CN] X) • Posterior cricoarytenoid: Abducts the vocal cords; recurrent laryngeal nerve (CN X) • Lateral cricoarytenoid: Adducts the vocal cords; recurrent laryngeal nerve (CN X) • Oblique arytenoid: Adducts the vocal cords, recurrent laryngeal nerve (CN X) • Transverse arytenoid: Adducts the vocal cords; recurrent laryngeal nerve (CN X) • Thyroarytenoid: Relaxes, shortens, and adducts the vocal cords; recurrent laryngeal nerve (RLN; CN X) |
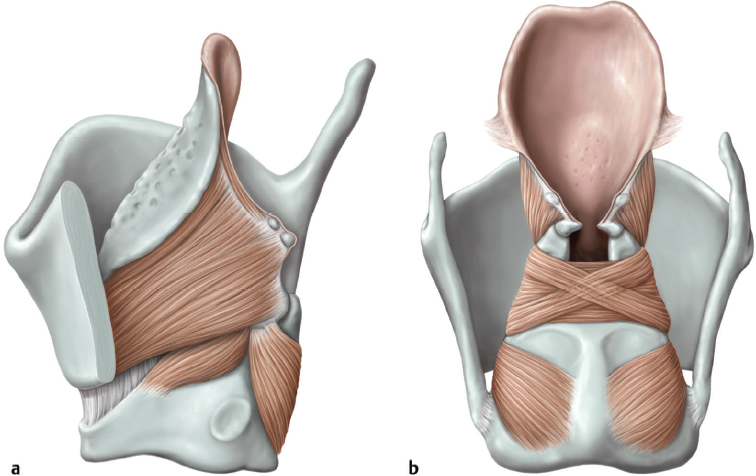
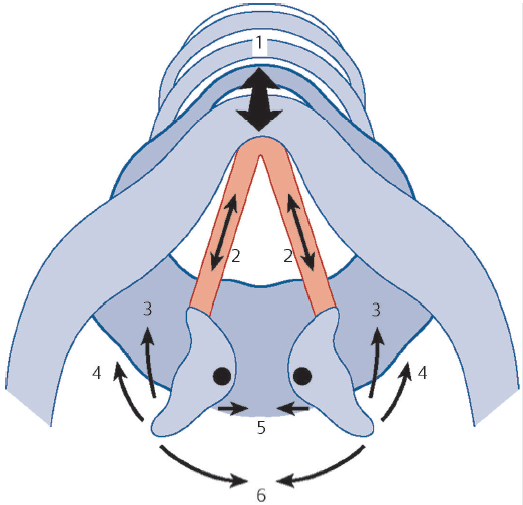
Fig. 5.2 Instrinsic muscles of the larynx and their directions of pull. (1) Cricothyroid muscle; (2) medial portion of the thyroarytenoid muscle; (3) lateral part of the thyroarytenoid muscle; (4) lateral cricoarytenoid muscle; (5) interarytenoid muscle; (6) posterior cricoarytenoid muscle. (Used with permission from Behrbohm H, Kaschke O, Nawka T, Swift A. Ear, Nose, and Throat Diseases: With Head and Neck Surgery. New York, NY: Thieme; 2009.)
What nerve provides sensation to the larynx? | CN X via the internal branch of the superior laryngeal nerve above the glottis and the recurrent laryngeal nerve below the glottis Glottic sensation is mainly from the superior laryngeal nerve with some sensory innervation from the RLN as well. | |
9 | What are the extrinsic muscles of the larynx, and what is their function and innervation? ( | • Sternohyoid: Caudal traction on the larynx; ansa cervicalis nerve • Sternothyroid: Caudal traction on the larynx; ansa cervicalis nerve • Omohyoid: Caudal traction on the larynx; ansa cervicalis nerve • Geniohyoid: Cephalad traction on the larynx; C1 via the hypoglossal nerve (CN XII) • Anterior belly of the digastric: Cephalad traction on larynx; nerve to the mylohyoid (V3) • Mylohyoid: Cephalad traction on the larynx; nerve to the mylohyoid (V3) • Stylohyoid: Cephalad traction on the larynx; facial nerve (CN VII) • Thyrohyoid: Caudal traction on larynx; ansa cervicalis nerve |
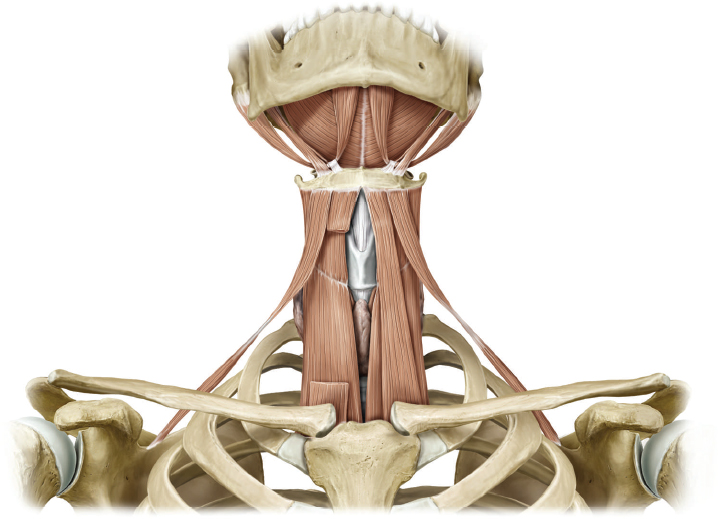
Fig. 5.3 Extrinsic muscles of the larynx: sternohyoid, sternothyroid, omohyoid, geniohyoid (not shown), anterior belly of the digastric, mylohyoid, stylohyoid, thyrohyoid. (Used with permission from Thieme Atlas of Anatomy: Head and Neuroanatomy, © Thieme 2007, illustration by Karl Wesker.)
Describe the subtypes of the laryngeal epithelium. | • Supraglottis: Pseudostratified columnar epithelium (respiratory epithelium) • Glottis: Stratified squamous epithelium • Subglottis: pseudostratified columnar epithelium (respiratory epithelium) • Lingual surface of the epiglottis: Stratified squamous epithelium • Laryngeal surface of the epiglottis: Stratified squamous merging into pseudostratified columnar epithelium | |
11 | What are the layers of the true vocal folds, from superficial to deep? ( | • Epithelium • Superficial lamina propria (SLP) • Intermediate lamina propria • Deep lamina propria • Thyroarytenoid muscle complex |
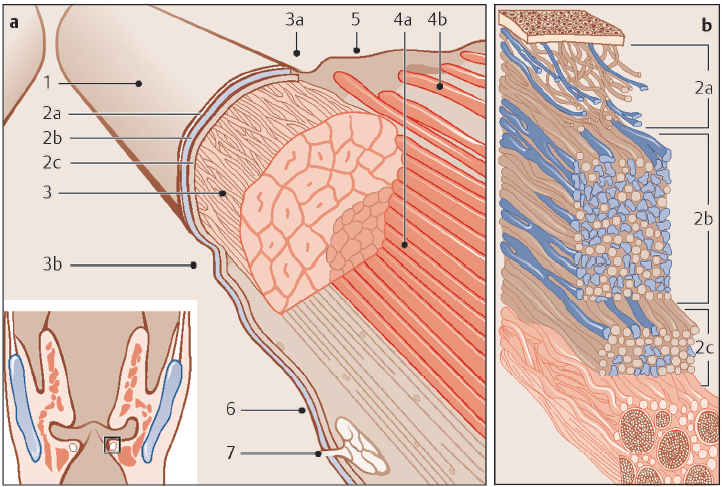
Fig. 5.4 Cross section through the membranous portion of the vocal fold. 1, Stratified squamous epithelium; 2a, superficial layer of the lamina propria; 2b, intermediate layer of the lamina propria; 2c, deep layer of the lamina propria, 2b and 2c forming the vocal ligament; 3, vocal ligament enveloping the vocalis muscle; 3a, superior arcuate line; 3b, inferior arcuate line; 4a, medial part of the thyroarytenoid muscle; 4b, lateral part of the thyroarytenoid muscle; 5, epithelium of the laryngeal ventricle (Morgagni ventricle); 6, subglottic respiratory cylindrical ciliated epithelial zone; 7, mucous gland. (Used with permission from Behrbohm H, Kaschke O, Nawka T, Swift A. Ear, Nose, and Throat Diseases: With Head and Neck Surgery. New York, NY: Thieme; 2009.)
12 | What layers form the vocal fold cover, ligament, and body, respectively, involved in the cover-body theory of voice production? | • Cover = epithelium + SLP • Ligament = intermediate lamina propria + deep layers of the lamina propria • Body = thyroarytenoid muscle |
Physiology of Speech and Voice
13 | True/False. A unilateral cortical stroke will always result in vocal-fold paralysis. | False. True vocal-fold motion is controlled by the brainstem via both pyramidal and extrapyramidal neural systems. The cell bodies of motor nerves reside within the nucleus ambiguus, whereas sensory nerves reside within the nodose ganglion. Therefore, cortical strokes rarely result in cord paralysis. |
14 | Vascular insult to what structure(s) may result in loss of pain/temperature sensation in the ipsilateral face and contralateral body, ipsilateral facial pain, ataxia, nystagmus, vertigo, nausea, vomiting, dysphonia, dysphagia, and Horner syndrome? ( | Vertebral artery or posterior inferior cerebellar artery (Wallenburg syndrome) |
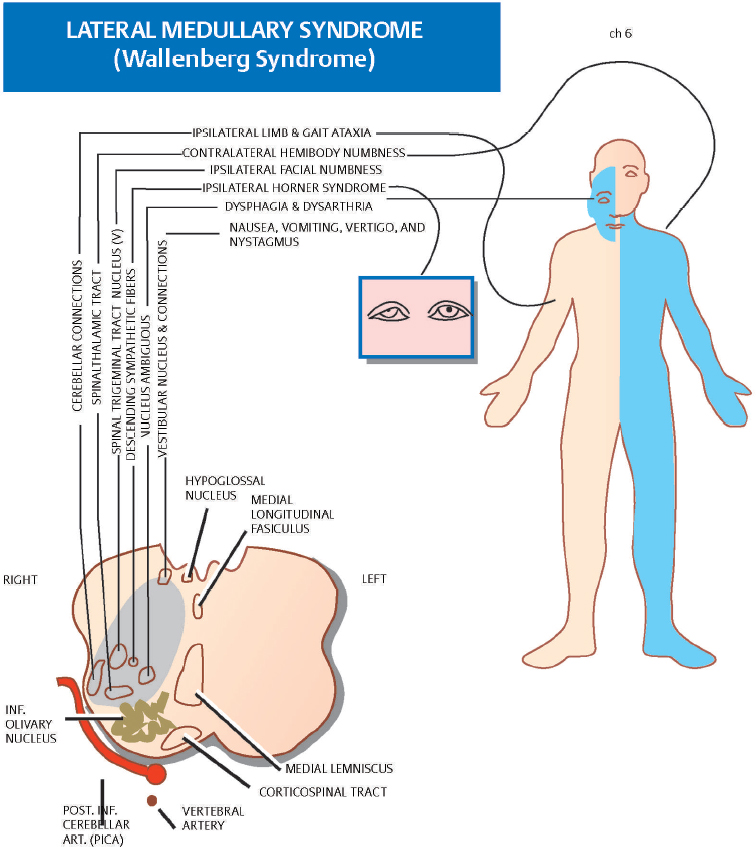
Fig. 5.5 Lateral medullary syndrome (Wallenburg syndrome) caused by a vascular insult to the vertebral artery or posterior inferior cerebellar artery. (Used with permission from Albertstone CD, Benzel EC, Najm IM, Steinmetz MP. Anatomic Basis of Neurologic Diagnosis. New York, NY: Thieme; 2009.)
The superior laryngeal nerve branches off the vagus nerve just caudal to what important neural structure? | The nodose ganglion | |
16 | What are the three levels of laryngeal airway protection? | Epiglottis False vocal folds True vocal folds |
17 | On physical examination, you note that a patient demonstrates a protective cough reflex with palpation of the tip of epiglottis but has no response to palpation of the lower laryngeal surface of the epiglottis or arytenoid mucosa. Which nerve is most likely injured? | Superior laryngeal nerve The tip of the epiglottis receives sensory innervation from the glossopharyngeal nerve (IX), and the lower epiglottis and arytenoid regions are innervated by the internal branch of the superior laryngeal nerve. |
18 | The laryngeal closure reflex can be driven by several different stimuli. Name four. | • Thermal • Mechanical • Chemical • Taste |
19 | During intubation, what hemodynamic response may occur due to laryngeal irritation? | Bradycardia and hypotension; cardiovascular collapse Circulatory laryngeal reflex (superior laryngeal nerve [SLN], perhaps RLN as well) →central neurons →vagus →heart) |
20 | What are the three types of laryngeal respiratory receptors? | • Negative pressure recep tors: Maintain airway patency during inspiration • Airflow receptors: Cold receptors, which are stimulated by air movement • Respiratory drive receptors: Provide laryngeal proprioception |
21 | What are three fundamental components of speech? | • Phonation: Vocal-fold vibration resulting in sound generation • Resonance: Modulation of laryngeal phonation by induction of vibration within the vocal tract • Articulation: Manipulation of the sound into words |
22 | What is required for voice production? | • Power: Adequate breath support (lungs) • Source of vibration: Larynx • Resonator: Supraglottic vocal tract and pharynx Note: Normal phonation requires a good vibratory medium; normal vocal-fold shape; and the ability to modify the tension, length, and shape of the true vocal folds. |
23 | How does injury to the superior laryngeal nerve impact voice production? | Loss of upper pitch register due to the loss of the motor innervation to the cricothyroid muscle via the external branch of the SLN, resulting in the inability to increase vocal tension |
24 | The intensity or loudness of sound production is directly related to air pressure in what location? | Subglottis |
25 | Describe the cover-body theory of voice production. | The cover (SLP) and body (thyroarytenoid muscle) move at different rates as air moves through the glottis because of their distinct masses and composition. This variation causes vibration, which results in a buzzing sound. The supraglottic vocal tract then modulates this sound to produce voice. |
26 | Pitch (or frequency) can be altered by adjusting the length and tension of the vocal fold. If this is done by contraction of the thyroarytenoid or cricothyroid muscle, what nerves are involved? | • Thyroarytenoid: RLN • Cricothyroid: External branch of the SLN |
Given a constant volume of airflow through the vocal tract, the airflow velocity will increase at the level of the true vocal folds. Increased velocity results in decreased pressure and an inward movement of the vocal folds. What name is given to this effect? | Bernoulli effect | |
28 | Describe the myoelastic-aerodynamic theory of voice production. | This was an early model of voice oscillation, which postulated that the Bernoulli effect would function to close the vocal folds, whereas increasing pressure in the subglottis from the lungs would function to open the vocal folds. This would occur over short bursts, resulting in a single puff of air being released. Sound production was thought to be a compilation of these puffs, dependent on the intensity of the sound source, the frequency of the source signal, and the supraglottic laryngeal tract. |
29 | What component of speech describes rhythm, repeated or prolonged syllables, rushes of speech, stress, and intonation? | Prosody |
Evaluation
30 | One of the first patient-based, voice-specific outcome measures was the Voice Handicap Index. This is a 30-question assessment that focuses on which three domains? | Functional, physical, and emotional aspects of voice disorders |
31 | Which voice-specific patient-reported outcome measure uses 10 questions to assess the physical functioning and social–emotional status of a patient with voice disturbance, and how is it measured? | The V-RQOL. Each question is given 1 to 5 points, with 5 representing a severe problem, and 1 representing no problem. An equation is then used to generate a score out of a total of 100, with a higher score representing better quality of life. |
32 | Name three important voice parameters. | • Frequency (pitch) • Intensity (loudness) • Quality (i.e., timbre) |
33 | What term refers to the number of repeating cycles per second (Hz) in the acoustic waveform? | Frequency |
34 | Define the fundamental frequency of the voice and the ranges for adult men and women. | The predominant pitch component of speech • Normal adult men into their 70s: 100 to 125 Hz • Normal adult women: 190 to 225 Hz |
35 | What describes the quality of a sound determined by its frequency (or fundamental frequency)? | Pitch |
36 | What acoustic term defines the loudness, or sound pressure level, of speech? | Intensity (normally 70 dB for both male and female conversational speech) |
37 | What factors most often influence loudness, or intensity? | Subglottic pressure, frequency, speech sample, glottal resistance, and airflow rate Type of equipment used, distance from the sound source, and ambient noise can also influence loudness measurements. |
38 | In acoustic analysis of voice, what are the most common parameters used to assess frequency? | • Average speaking fundamental frequency • Maximum phonational frequency range |
39 | What describes the quality or character of voice, separate from pitch, intensity, and prosody? | Quality (timbre): Roughness, breathiness, and strain |
40 | What is the perceptual correlate of the frequency of a sound wave? | Pitch (perceptual correlate of frequency) |
41 | What is the perceptual correlate of the amplitude of a sound wave? | Volume is the perceptual correlate of amplitude. |
In acoustic analysis of voice, jitter is defined as cycle-to-cycle variation in what parameter? | Frequency of a wave (normal = 0.40%) | |
43 | In acoustic analysis of voice, shimmer is defined as cycle-to-cycle variation in what parameter? | Amplitude of a wave (normal = 0.50 dB). |
44 | What are the most common measurements used to assess voice quality in acoustic analysis of voice? | Short-term perturbation measures (only reliable for nearly periodic signals): • Jitter: Cycle-to-cycle variation in frequency • Shimmer: Cycle-to-cycle variation in amplitude Note: No single test has been identified to reliably assess voice quality. |
45 | The GRBAS scale is an assessment tool, which attempts to standardize the auditory perceptual evaluation of voice quality. What does GRBAS represent, and how is this assessment scored? | G Grade: Overall severity R Roughness: Psychoacoustic impression of irregular vocal-fold vibration B Breathiness: Psychoacoustic impression of air leakage through the glottis A Asthenia: Weakness or lack of power in the voice S Strain: Psychoacoustic impression of hyperfunctional state of phonation 0: No deficit in parameter 1: Mild deficit 2: Moderate deficit 3: Severe deficit |
46 | What is the major weakness of the GRBAS scale? | It does not offer a specific protocol for administration or guidelines for analysis. |
47 | Which auditory-perceptual evaluation tool uses a visual analog scale (100-mm line; increasing distance from the left indicates increasing severity) to assess six parameters of voice: overall severity, roughness, breathiness, strain, pitch and loudness, and how is it scored? | Consensus Auditory-Perceptual Evaluation-Voice (CAPE-V): The score is based on two sustained vowels, six standard sentences, and 20 or more seconds of natural running speech. The six parameters are evaluated for resonance differences and whether the parameter is constant or intermittent. |
48 | Define the following terms: 1. Aphonia 2. Breathy voice 3. Diplophonia 4. Dysphonic 5. Flutter 6. Hoarse voice 7. Hypernasal (honky, nasal) 8. Hyponasal 9. Resonant 10. Strained (harsh, strangled) 11. Tremor | 1. The inability to set the vocal folds into vibration either consistently or intermittently. Note: Arrest of phonation describes sudden stops. 2. Containing the sound of breathing (expiration) during phonation 3. Phonation with two independent pitches 4. Abnormal phonation 5. Phonation with amplitude or frequency modulations in the 8- to 12-Hz range 6. The combination of a rough and breathy voice 7. Voice quality when excessive acoustic energy is coupled to the nasal tract through opening of the velar port 8. Voice quality when inadequate acoustic energy is coupled to the nasal tract 9. A voice quality that rings on or “carries” well 10. A voice quality that appears effortful 11. A 1- to 15-Hz modulation of a cyclic parameter (e.g., amplitude or fundamental frequency), either neurologic in origin or interaction between neurologic and biomechanical properties |
49 | An important adjunct to the auditory-perceptual evaluation of the dysphonic patient is the visual-perceptual evaluation, which evaluates visible and physical facets of voice production related to cause, maintenance, or effect of dysphonia. What five categories are evaluated? | • General appearance • Posture, breathing, musculoskeletal tension • Neurologic dysfunction • Physical dysmorphology • Clinical manifestations of disease |
When assessing a patient who has dysphonia suspicious of muscle tension or muscle misuse dysphonia, what tactile-perceptual tests can be completed in the office to provide a clinical assessment of dysfunction? | • Palpation of the suprahyoid, thyrohyoid, cricothyroid, and pharyngolaryngeal muscles both at rest and during phonation • Assessment of the thyrohyoid space for anterosuperior supraglottic compression • The clinician should assess for tension, muscle “knots,” decreased space between thyroid cartilage and hyoid, or discomfort on mobilization. | |
51 | What is the aerodynamic assessment that measures the length of time a patient can sustain a vowel after having taken a maximum inspiration? | Maximum phonatory time (indicates breath support and phonatory efficiency The longest of three trials should be reported. Typically, adult women range between 15 and 25 seconds, adult men between 25 and 35 seconds. |
52 | The subglottic air pressure (force/unit area) can be evaluated clinically by measuring the intraoral air pressure during a voiceless consonant. What influences the magnitude of normal pressure peak variation, and what are normative values for men and women? | Loudness, age, gender, consonant, and speech context • Men: 7.52 cm H2O • Women: 6.43 cm H2O |
53 | What term describes the minimal subglottic pressure needed for vocal fold vibration? | Phonation threshold pressure |
54 | Define transglottic airflow and its gender-specific ranges. | Transglottic airflow is the volume of air that passes through the glottis during a specific period. It can be traced during sustained phonation or connected speech and is associated with breathiness. • Men: 100 to 183 mL/second • Women: 91 to 156 mL/second |
55 | What is the term given to the ratio of translaryngeal air pressure to translaryngeal airflow? What are the normative values in each gender, and what is the perceptual correlate? | Laryngeal airway resistance • Men: 25 to 45 cm H2O/L/second • Women: 27 to 51 cm H2O/L/second Phonatory effort, vocal strength, strain |
56 | What test measures the conductance of low-frequency electrode signals between two surface electrodes on the neck to assess vocal fold vibration? | Electroglottography |
57 | What is the maximum number of images the retina can distinguish per second, and how does this compare with the rate of vocal fold vibration? | • Retina: Five images per second (Talbot’s law) • Vocal cords: 75 to 1,000 cycles per second Therefore, vocal-fold vibration cannot be seen by the naked eye. |
58 | Videostroboscopy uses a xenon light with rapid on-and-off bursts to view the larynx in brief snapshots, fusing images, and “slowing” the motion of the vibration. This allows for visualization by the human retina. Why does videostroboscopy require a microphone? | The microphone is placed on the patient’s neck to sense laryngeal vibration, which in turn controls the rate of xenon light firing. Light activation must be out of phase with laryngeal vibration to identify movement. |
59 | What five important criteria are used to grade videostroboscopy? | • Symmetry • Periodicity • Amplitude • Mucosal wave • Closure |
60 | Define the following terms: • Symmetry • Periodicity • Amplitude • Mucosal wave • Closure | • Symmetry: Mirrorred appearance of the two vocal folds • Periodicity: Regularity of successive glottal cycles • Amplitude: Lateral excursion of the midmembranous cord • Mucosal wave: Vertical and horizontal movement of the cover (SLP) over the body (thyroarytenoid muscle) • Closure: Closure of the cartilaginous and membranous portions of the glottis |
61 | During videostroboscopy on a normal patient, the mucosal wave will be seen traveling over what fraction of the superior portion of the true vocal fold? | From the inferior lip of the true vocal fold up the medial edge and across approximately one-half of the superior surface |
62 | True or False. Videostroboscopy is an excellent tool in the evaluation of all voice pathologies, including those without periodic vibration of the true vocal folds. | False. Videostroboscopy can analyze only periodic vocal-fold vibration. |
63 | What is the main advantage of videokymography over videostroboscopy? | Videokymography captures multiple images of a single glottic cycle, allowing for analysis of aperiodic vocal-fold vibration. Videostroboscopy is effective only in the setting of periodic vocal-fold vibration and provides an averaging of images. |
64 | What describes altered vocal quality, pitch, loudness, communication, or voice-related quality of life? | Dysphonia |
65 | What are common risk factors for dysphonia (hoarseness)? | • Upper respiratory tract infection • Recent or current infection • Significant voice use, misuse, or abuse • Recent neck trauma • Recent surgery (e.g., airway, neck or thoracic surgery) • Recent intubation • Tobacco and alcohol use • Reflux • Neurologic disorders • Psychiatric illness or stress • Hypothyroidism • Recent choking or foreign-body aspiration/ingestion |
66 | What type of stridor would be seen in (1) supraglottic, (2) glottic, (3) subglottic, or (4) tracheobronchial airway obstruction? | 1. Inspiratory 2. Inspiratory or biphasic 3. Biphasic 4. Expiratory |
67 | When a suspected aspiration event has occurred, describe the most important aspects of the history and evaluation in a stable patient. | SPECS-R* S: Severity of obstruction on clinical exam P: Progression of obstruction E: Eating difficulty, failure to thrive C: Cyanotic episodes S: Sleep disturbance – R – Radiographic abnormalities (only obtain if information will change management and patient is not in acute distress) *Clinical suspicion: Witnessed aspiration, etc. |
Nonoperative Therapy
68 | When is voice therapy alone an appropriate treatment option for patients with dysphonia? | When medically and surgically treatable causes have been ruled out and a patient continues to have decreased voice related quality of life |
69 | When should antireflux medications be prescribed for hoarseness (dysphonia)? | Only when there are signs or symptoms of reflux disease or chronic laryngitis |
70 | True or False. Proton Pump Inhibitors (PPIs) may cause dysphonia in some patients. | True. PPI use can cause laryngeal dryness and candidiasis leading to dysphonia. |
Why should the histamine 2 (H2) receptor antagonists cimetadine and ranitidine be prescribed with caution in patients taking either tricyclic antidepressants or benzodiazepines? | Cimetadine and, to a lesser extent, ranitidine inhibit the cytochrome p450 enzymes that metabolize these medications and can lead to increased blood levels. | |
72 | What are the most common side effects of PPI therapy? | Abdominal pain, diarrhea, nausea, vomiting, elevated liver function tests, candidiasis, headache, osteoporosis |
73 | Which asthma medications are associated with voice changes? | Inhaled and systemic steroids, β-agonists, and anticholinergics |
74 | Why should thyroid hormone levels be monitored in professional voice users? | Hypothyroidism may cause voice changes. |
75 | Describe the voice changes associated with hormonal therapy (androgens, estrogen, progesterone). | Lower fundamental frequency and increased roughness |
76 | Describe the difference between indirect and direct voice therapy. | Indirect voice therapy focuses on improving vocal hygiene and decreasing phonotrauma. Direct voice therapy focuses on improving voice production. |
77 | What voice therapy technique has been proven to improve speech and speech-related activities in patients with Parkinson disease? | Lee Silverman voice therapy (LSVT) |
Benign Disorders
78 | Damage to the vocal folds resulting from voice abuse, misuse, and overuse can give rise to various vocal-fold lesions. This type of damage is called _____? | Phonotrauma |
79 | What is the most common location of true vocal fold lesions resulting from voice abuse? | Mid-membranous vocal fold |
80 | What is the term for benign growths in the superficial layer of the anterior and middle third of the true vocal fold, which can be either acute (edematous, erythematous, more vascular) or chronic (firm, nonvascular, thickened due to scar deposition and fibrosis)? | Vocal-fold nodules |
81 | What is the most common cause of vocal fold nodules? | Phonotrauma (ex: singing, screaming) |
82 | Before any surgical intervention for vocal-fold nodules, what is the first line of management? | Voice therapy |
83 | In addition to voice therapy, what two contributing medical conditions should be optimized when treating a patient with vocal fold nodules? | • Laryngopharyngeal reflux • Allergies |
84 | Describe the pathophysiologic sequence that gives rise to vocal fold nodules. | Excessive vibration causes trauma leading to vascular congestion and submucosal edema at the midmembranous cord. If the vocal trauma continues, hyalinization of the superficial lamina propria and epithelial thickening may occur. |
85 | When is it appropriate to consider surgical removal of vocal-fold nodules? |



