Laryngeal carcinoma is the eleventh-most common form of cancer among men worldwide and is the second-most common malignancy of the head and neck. The primary functions of the larynx involve phonation, respiration, and deglutition but it also contributes to taste and smell by allowing the movement of air over the special sense organs. Thus, loss of laryngeal function affects speech and swallowing and some of the senses that allow us to enjoy the world. Moreover, total laryngectomy bypasses the critical humidification function of the upper aerodigestive tract that renders pulmonary toiletry problematic for these patients. With relatively little change in mortality since the 1970s, recent research has focused not only on improving survival but on laryngeal preservation modalities.
Laryngeal carcinoma is the eleventh-most common form of cancer among men worldwide and is the second-most common malignancy of the head and neck. In the United States in 2007 there were an estimated 11,300 new cases of laryngeal cancer and 3,600 cases of disease-specific mortality . The primary functions of the larynx involve phonation, respiration, and deglutition but it also contributes to taste and smell by allowing the movement of air over the special sense organs. Thus, loss of laryngeal function affects speech and swallowing and some of the senses that allow us to enjoy the world. Moreover, total laryngectomy bypasses the critical humidification function of the upper aerodigestive tract that renders pulmonary toiletry problematic for these patients. With relatively little change in mortality since the 1970s, recent research has focused not only on improving survival but on laryngeal preservation modalities.
Prevention and early diagnosis of laryngeal carcinoma is the most effective means for maximizing cure rates and preserving function. Fortunately, glottic laryngeal carcinoma, the most common laryngeal tumor, tends to be detected at an earlier stage than tumors located at other subsites of the head and neck. Nevertheless, the symptoms of laryngeal carcinoma can also be nonspecific and may result in a delay of diagnosis. In general, hoarseness lasting longer than 3 weeks or odynophagia or dysphagia lasting longer than 6 weeks should warrant a referral to an otolaryngologist—especially for patients older than 50 years with an extensive smoking or drinking history. Associated otalgia, stridor, and weight loss should also be red flags to completely rule out a malignant process.
The preoperative evaluation of patients with laryngeal carcinoma begins with a thorough history and physical examination in the office with subsequent endoscopy and surgical biopsy for tissue diagnosis. Once a diagnosis is made, the physician and patient must together formulate an individualized plan based on the tumor characteristics as well as the patient’s wishes. In McNeil’s frequently quoted study of firemen and upper management executives with advanced laryngeal cancer, one of five patients would accept a 20% to 30% decrease in survival to preserve their voice . This study clearly demonstrates that patients place a significant premium on quality of life and that clinicians cannot perseverate on maximizing survival alone. Another critical issue in the formulation of a treatment plan is an open discussion regarding some of the recent findings of short-term and long-term quality of life in patients who have undergone partial and total laryngectomies as well as endoscopic partial laryngectomies.
Biology of laryngeal malignancy
Effective treatment and understanding of laryngeal cancer requires fundamental knowledge of the complex anatomy of this region. Based on its embryologic development, the larynx can be divided into three levels: supraglottic, glottic, and subglottic, with each level containing a number of subsites ( Table 1 ). These divisions have clinical relevance in that they help predict the clinical behavior and pattern of spread of the tumor.
| Level | Subsites |
|---|---|
| Supraglottis | Suprahyoid epiglottis (tip, lingual, and laryngeal surfaces) |
| Aryepiglottic fold | |
| Arytenoids | |
| Infrahyoid epiglottis | |
| False cords | |
| Glottis | True vocal folds |
| Anterior commisure | |
| Posterior commisure | |
| Subglottis |
The supraglottis extends from the tip of the epiglottis superiorly to the apices of the ventricles and undersurface of the false cords and includes both the lingual and laryngeal surfaces of the epiglottis, the arytenoid cartilages, the aryepiglottic (AE) folds, and the false cords. The supraglottis develops from the midline buccopharyngeal anlage from branchial arches 4 and 6 with rich bilateral lymphatics. Clinically, this translates to a significant incidence of unilateral or bilateral cervical metastasis—25% to 75% for all T-stages .
The glottic larynx encompasses the floor of the ventricle, the true vocal folds extending to 0.5 cm below the free edge of the cord, the anterior commisure, and the interarytenoid area. In contrast to the supraglottic structures, the glottis forms from the midline fusion of lateral structures derived from the tracheobronchial anlage from arches 4, 5, and 6 and has a relative dearth of lymphatics. Consequently, this embryologic boundary limits submucosal spread to adjacent sites within the larynx for early stage cancers, and the paucity of lymphatic in the glottis contains lymphatic spread to the neck allowing glottic cancers to remain localized to the larynx for longer periods of time.
The subglottis continues from the inferior limit of the glottis to the inferior edge of the cricoid cartilage. It develops from the fourth and sixth pharyngeal arches and because of its location has a propensity for extralaryngeal extension.
Laryngeal framework
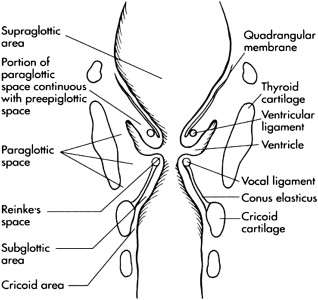
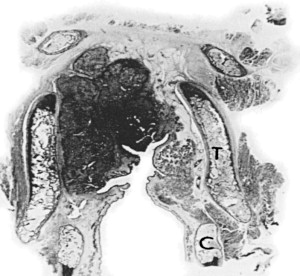
Except for advance stage tumors, most laryngeal cancers tend to remain confined to one anatomic site because of the “pushing” mechanism of tumor growth ( Fig. 1 ). Seminal dye and histologic studies have confirmed this compartmentalization in lymphatics and vasculature . Additionally, cartilaginous and fascial anatomic structures, such as the thyroid and cricoid cartilages with their overlying perichondrium, the ventricle, the conus elasticus, the quadrangular and thyrohyoid membranes, and the hyoepiglottic ligament, act as barriers to spread ( Fig. 2 ). The anterior commisure and thyrohyoid membrane, in contradistinction to the above structures, offers little resistance to tumor spread. For the purpose of TNM staging, knowledge of these anatomic ligaments and potential spaces may not be helpful; however, in the overall evaluation of laryngeal malignancy, framing the work-up of the lesion in the context of these barriers is critical in providing the optimal diagnosis and therapy for the patient.
Laryngeal spaces (potential)
Pre-epiglottic space
These fibroelastic membranes and ligaments define two critical potential spaces around the larynx. The pre-epiglottic space is bound superiorly by the hyoepiglottic ligament, anteriorly by the thyroid cartilage and thyrohyoid membrane, and posteriorly by the epiglottis and thyroepiglottic ligament. The cartilage of the epiglottis has numerous perforations that allow transit of tumor from the posterior surface of the epiglottis into the pre-epiglottic space. Furthermore, dehiscences in the thyrohyoid membrane created by the superior laryngeal neurovascular bundle allow extension of tumor from the pre-epiglottic space into the neck.
Paraglottic space
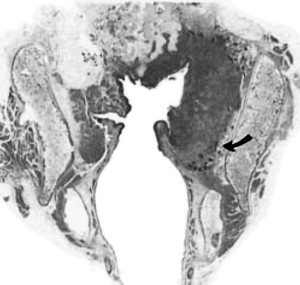
Alternatively, tumor may invade in a cephalad-caudal spread via the paraglottic space into all the subsites of the larynx ( Fig. 3 ). The paraglottis space is a potential space, and together with the pre-epiglottic space forms, a horseshoe-shaped fatty space around the internal laryngeal structures. The lateral boundaries of the paraglottic space are the thyroid cartilage anteriorly and the mucosa overlying the medial wall of the piriform sinus posteriorly. Superiorly and medially lie the quadrangular membrane, and the conus elasticus is situated inferiorly. Involvement of the paraglottic space by tumor allows fascial free access to the supraglottic, glottic, and subglottic regions in addition to the soft tissues of the neck. Transglottic tumors by definition involve the paraglottic space superior and inferior to the ventricle (see Fig. 3 ).
Laryngeal framework
Except for advance stage tumors, most laryngeal cancers tend to remain confined to one anatomic site because of the “pushing” mechanism of tumor growth ( Fig. 1 ). Seminal dye and histologic studies have confirmed this compartmentalization in lymphatics and vasculature . Additionally, cartilaginous and fascial anatomic structures, such as the thyroid and cricoid cartilages with their overlying perichondrium, the ventricle, the conus elasticus, the quadrangular and thyrohyoid membranes, and the hyoepiglottic ligament, act as barriers to spread ( Fig. 2 ). The anterior commisure and thyrohyoid membrane, in contradistinction to the above structures, offers little resistance to tumor spread. For the purpose of TNM staging, knowledge of these anatomic ligaments and potential spaces may not be helpful; however, in the overall evaluation of laryngeal malignancy, framing the work-up of the lesion in the context of these barriers is critical in providing the optimal diagnosis and therapy for the patient.
Laryngeal spaces (potential)
Pre-epiglottic space
These fibroelastic membranes and ligaments define two critical potential spaces around the larynx. The pre-epiglottic space is bound superiorly by the hyoepiglottic ligament, anteriorly by the thyroid cartilage and thyrohyoid membrane, and posteriorly by the epiglottis and thyroepiglottic ligament. The cartilage of the epiglottis has numerous perforations that allow transit of tumor from the posterior surface of the epiglottis into the pre-epiglottic space. Furthermore, dehiscences in the thyrohyoid membrane created by the superior laryngeal neurovascular bundle allow extension of tumor from the pre-epiglottic space into the neck.
Paraglottic space
Alternatively, tumor may invade in a cephalad-caudal spread via the paraglottic space into all the subsites of the larynx ( Fig. 3 ). The paraglottis space is a potential space, and together with the pre-epiglottic space forms, a horseshoe-shaped fatty space around the internal laryngeal structures. The lateral boundaries of the paraglottic space are the thyroid cartilage anteriorly and the mucosa overlying the medial wall of the piriform sinus posteriorly. Superiorly and medially lie the quadrangular membrane, and the conus elasticus is situated inferiorly. Involvement of the paraglottic space by tumor allows fascial free access to the supraglottic, glottic, and subglottic regions in addition to the soft tissues of the neck. Transglottic tumors by definition involve the paraglottic space superior and inferior to the ventricle (see Fig. 3 ).
Office evaluation
The are three major goals to the initial evaluation:
- (1)
Determining whether or not the lesion is malignant (tissue diagnosis)
- (2)
Staging the lesion in the context of the optimal treatment for the patient
- (3)
Mapping both the gross disease and regional nodes as well as potential occult or metastatic disease.
The typical patient is a male in his 50s or 60s with a history of smoking and alcohol use. However, the male predilection for this disease has recently decreased from a male:female ratio of 15:1 to currently less than 5:1 . This change in demographics has been attributed to increased rates of smoking among females and their increasing presence in equally toxic work environments. Significant variation in the distribution of carcinoma at the different laryngeal subsites exists worldwide. Supraglottic and glottic tumors are the most prominent subsites, and subglottic carcinomas are uniformly rare. In the United States, glottic carcinomas are the most common (glottic, 59%; supraglottic, 40%; subglottic, 1%) . However, given the heterogeneity of ethnic and immigrant population in the North American cities, clinical suspicion for uncommon subsites as well as risk factors related to ethnic diet and customs should be considered.
History
As with all head and neck malignancies, the evaluation begins with a thorough history. This should include not only a careful review of the chief complaint but also an assessment of associated medical problems, social history (specifically amount and duration of tobacco and alcohol use), family history of all types of malignancies, and a complete review of symptoms with an eye toward any symptoms suggestive of metastatic involvement. Careful review of the patient’s history and symptoms can often give insight into the location and extent of the disease.
Typical symptoms include hoarseness, dysphagia, odynophagia, neck mass, referred otalgia, dyspnea, and aspiration. Since minor changes to the vocal fold affect the mucosal wave and result in hoarseness, it comes as no surprise that glottic tumors tend to be diagnosed at an earlier stage than supraglottic or subglottic cancers. Hoarseness in the latter two instances would suggest a more advanced lesion with spread to either the cricoarytenoid unit or deep invasion into the laryngeal musculature. It is important to note that patients with reflux laryngitis and heavy smoking history may have a chronically inflamed larynx at baseline and may not appreciate subtle changes in their voice. Dyspnea could be a result of either significant vocal fold motion impairment or bulky disease while dysphagia and odynophagia suggest possible involvement of the tongue base or hypopharynx.
Supraglottic tumors
In contrast to glottic tumors, supraglottic tumors often come to the attention of a head and neck surgeon only after persistent symptoms of dysphagia, odynophagia, and otalgia. Because of the nonspecific nature of their symptoms, these patients have frequently already seen other physicians who have treated them with medical therapies without a clear diagnosis. At the time of presentation, many patients have already developed palpable neck disease and significant weight loss.
Subglottic tumors are rare and often present in the emergent setting with airway obstruction or vocal fold paralysis. Hypopharyngeal malignancies, which are less common in the United States, also present as advanced disease with comparable symptoms as supraglottic lesions with related risk factors such as tobacco use and extensive alcohol use. Aside from postcricoid carcinoma, hypopharyngeal tumors also present in men with a heavy smoking and drinking history. Women of European descent with chronic dysphagia and history of Plummer-Vinson syndrome should also be a red flag in the evaluation for hypopharyngeal lesions, particularly postcricoid subsite.
Etiology
Tobacco and alcohol abuse
Eighty-five percent of laryngeal cancers can be attributed to tobacco and alcohol use. Smoking is the predominant risk factor for laryngeal carcinoma with alcohol use being an independent and synergistic risk factor . Current smokers have a 10- to 20-fold increased risk of laryngeal cancer compared with nonsmokers . However, these risks decline sharply after smoking cessation—although never to the same level as patients who have never smoked. Ten to 15 years after smoking cessation, there is an approximately 60% reduction in relative risk. While smoking cessation is the single most effective means of preventing laryngeal cancer, it is equally important to encourage patients to quit smoking after the diagnosis of laryngeal cancer has been made. Smoking has been identified as an independent risk factor for local recurrence and for recurrence at an earlier time point than those who ceased smoking .
Other risk factors include carcinogens in the workplace such as asbestos, nickel compounds, wood dust, leather products, paint, diesel fume, and glass-wool . Additionally, there is a controversial association with chronic gastroesophageal reflux as well as an increased incidence of squamous cell carcinoma in preexisting laryngeal respiratory papillomatosis. While there is good evidence for a causal link between human papillomavirus (HPV) subtypes 16 and 18 and oropharyngeal cancer, the association with laryngeal cancer is not as robust .
Comprehensive medical history
Patients with a prior history of a head and neck malignancy have an approximately 14% chance of developing a second primary malignancy in the head and neck. It is important to review the patient’s past medical history not only for prior malignancies but also for conditions that may warrant extra preoperative work-up, ie, significant coronary artery disease or chronic obstructive pulmonary lung disease. Clinical pulmonary function assessment is critical in the choice of treatment since baseline pulmonary reserve partly dictates the success of conservation laryngeal surgery. An assessment of the patient’s motor ability helps predict the likelihood of success with a tracheo-esophageal prosthesis for voicing. Additionally, based on the patient’s history and examination, nutrition and dental consultation should be considered as needed.
Finally, the patient’s social history should be considered in as much as it can influence treatment decisions. For example, two patients with identical-stage tumors but one whose livelihood is dependent on his or her voice and the other a patient who is a social recluse with limited transportation capability, may each benefit from different treatment plans. According to the preeminent clinician, Osler, this is a classic situation where the physician should “treat the patient,” and not the disease.
Physical examination
The overall goals of the office examination are to assess the extent of tumor involvement, vocal cord mobility, airway patency, and the extent of locoregional spread. To this end, a complete head and neck examination, including examination of all mucosal surfaces, is essential, especially given the 4% to 8% incidence of synchronous lesions in upper aero-digestive tract in patients with head and neck malignancies. Visualization of the larynx by either mirror and/or endoscopic examination is mandatory.
All regions above the clavicle are carefully palpated for evidence of metastatic disease or direct extralaryngeal extension. All too often, clinical examination on the lateral aspect of the neck is extensively documented without a careful assessment of the midline structures. Loss of the normal crepitance with side-to-side movement of the laryngeal framework may indicate postcricoid involvement. Complete fixation of the laryngeal complex on clinical examination is also suggestive of prevertebral involvement. Careful palpable assessment of the thyrohyoid membrane, thyroid cartilage, and cricothryoid membrane, as well as the overlying soft tissue of the laryngeal complex may provide a more clinically useful assessment of the tumor than any advanced imaging analysis. Laryngeal carcinoma most frequently metastasizes to nodal levels II, III, and IV in the neck. Supraglottic tumors have the highest rates of occult cervical metastasis: T1, 20%; T2, 40%; T3, 60%; and T4, 80%. Early glottic lesions have a less than 7% incidence of occult metastasis but T4 lesions can have up to a 40% incidence . Physical examination directed toward central compartment lymphatic spread (Delphian nodes) must not be ignored. Subglottic tumors have a significant incidence of extralaryngeal spread because of their proximity to the cricothyroid membrane and the rich postcricoid lymphatics. However, the true incidence of occult metastasis for subglottic disease is difficult to determine because of the rarity of the disease.
Pulmonary status
The patient’s pulmonary status will help determine the timing of planned surgical endoscopy and the need for possible tumor debulking versus tracheostomy. Audible stridor and use of accessory muscles during breathing at rest may require an urgent or emergent surgical airway. Pulmonary function tests and a careful review of the patient’s exercise tolerance (ie, can he or she walk up two flight of stairs without stopping?) are especially important if conservation surgery is being contemplated because the patient’s preoperative pulmonary reserve is an important indicator of how well the patient will tolerate aspiration postoperatively. Nevertheless, no objective standards exist that can reliably distinguish which patients are able to tolerate the physiologic changes accompanying conservation laryngeal surgery.
Laryngoscopy
Office-based laryngoscopy should answer several questions. First and foremost is to look for any lesions. The critical sites to evaluate are base of tongue, valleculae, epiglottis, aryepiglottic folds, arytenoids, interarytenoid regions, false cords, ventricles (if possible), true cords, subglottis (if possible), and some of the subsites of the hypopharynx. Extensive pooling of saliva in the piriform sinus and the larynx should be noted as a subtle sign for other occult pathology. Last, laryngoscopy should be used to assess the gross appearance and growth pattern (exophytic versus submucosal) since this may raise the suspicion for skip lesions, occult disease, subclinically extensive tumor, or nonsquamous pathology.
Indirect mirror laryngoscopy provides an excellent overview of the larynx and tongue base as well as excellent color and depth perception. However, it is often difficult to visualize the anterior commisure, especially in patients with a strong gag reflex.
Flexible fiber-optic laryngoscopy (FFL), possibly combined with stroboscopy, allows a closer look at individual areas and allows for video and photographic documentation of any visible pathology in a physiologic setting. Patients often appreciate being able to directly visualize the lesion on the monitor and it may facilitate their understanding of the disease process. The office examination provides the best opportunity to assess vocal fold movement as well as movement of the cricoarytenoid joint. Maneuvers, such as having the patient cough lightly, may help elucidate arytenoid mobility or lack thereof.
It is critical to distinguish between a true fixed vocal fold due to paraglottic space invasion versus cricoarytenoid joint involvement by the tumor. Bilateral arytenoid immobility secondary to cricoarytenoid involvement with tumor is a contraindication to organ preservation surgery. The extent of the tumor or suspicious areas for biopsy will aid the planning of the operative laryngoscopy and biopsy. With adequate topical anesthesia, the flexible fiber-optic laryngoscope can be passed through the cords to visualize the subglottis. Evaluation of the patency of the airway combined with vocal fold function can prevent unforeseen difficulties with subsequent intubation.
Rigid endoscopic evaluation
Rigid 70° or 90° endoscopes provide a similar view as with indirect mirror laryngoscopy but with added magnification. Similar to FFL, rigid endoscopes when combined with a stroboscopic light source allows for excellent visualization of the mucosal wave and may aid in detecting early glottic lesions by subtle changes in mucosal wave dynamics. Extrusion of the tongue required for rigid endoscopy may place the larynx in a slight nonphysiologic position, but the wealth of clinical information it provides outweighs theoretic arguments against its use. The practical worries of patients with strong gag reflex can be resolved with practical experience.
The current standard of care calls for biopsies in the operating room during surgical endoscopy; however, sheaths with working channels are now available that fit over existing flexible fiber-optic laryngoscopes allowing for in-office transnasal endoscopic biopsies (MedtronicENT, Inc, Jacksonville, Florida). In fact, use of transnasal laryngoscopy and esophagoscopy may facilitate or substitute the operative panendoscopy in select cancer patients. In a prospective study of 17 patients, Postma and colleagues found transnasal endoscopic biopsy results to be entirely congruent with standard panendoscopy biopsies taken in the operating room. The biopsies obtained via transnasal endoscopy were diagnostic for cancer in 12 of 12 patients and negative for malignancy in 5 of 5.
TNM staging dictates that true vocal cord mobility is properly assessed for proper staging according to American Joint Committee on Cancer (AJCC). However, it should be highlighted that the cricoarytenoid unit is the basic functional unit of the hemilarynx, and the visible abnormal mobility of the true cords should be assessed with this in mind. The function of the cricoarytenoid unit dictates whether the patient is a candidate for organ preservation surgery. The fixation of the involved cords on office-based laryngoscopy may stage the patients as T3, but this does not sufficiently assist in the treatment plan. Furthermore, the possibility of pseudofixation because of bulky mass effect on the arytenoids should be assessed whenever possible.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


