, Vincent Y. W. Lin2 and Joseph M. Chen2
(1)
Department of Otorhinolaryngology, Medical University of Vienna, Vienna, Austria
(2)
Department of Otolaryngology Head & Neck Surgery, Sunnybrook Health Sciences Center, Toronto, Ontario, Canada
Electronic supplementary material
Supplementary material is available in the online version of this chapter at 10.1007/978-3-7091-1490-2_11. Videos can also be accessed at http://www.springerimages.com/videos/978-3-7091-1489-6.
Completely drilling out the semicircular canals and removing all the soft tissue of the canals and the vestibule is referred to as labyrinthectomy. The indication for this procedure is the eradication of labyrinthine vertigo which is a hallmark symptom of conditions such as Meniere’s disease. In addition, it is a common (non hearing preserving) surgical route to the internal auditory canal (IAC) and cerebellopontine angle (CPA).
Prior to the labyrinthectomy, a cortical mastoidectomy is first carried out which is then followed by the identification of the facial nerve and all three semicircular canals (SCC). To reach this goal, a wide exposure of the middle and posterior dural plate as well as a complete drill-out of the sinodural angle is necessary. Only in this way, both the neurotologist and neurosurgeon will have enough space (instruments and light) to work deep in the CPA and IAC. Therefore, the term “medial temporal bone resection” for this approach describes very well the extensive amount of bone removal that is necessary for an appropriate exposure.
For a labyrinthectomy, the semicircular canals should be drilled out in a systematic fashion to identify the vestibule of the inner ear (Videos 7 and 8).
The initial step is usually opening the superior side of the lateral (horizontal) semicircular canal using a sharp cutting burr. A burr of 3-mm is a perfect size for this step. The canal should be slowly opened until the membranous labyrinth can be seen (“blue lining”; Fig. 11.1). Work in a front-to-back fashion. Proceed to open the lateral semicircular canal.
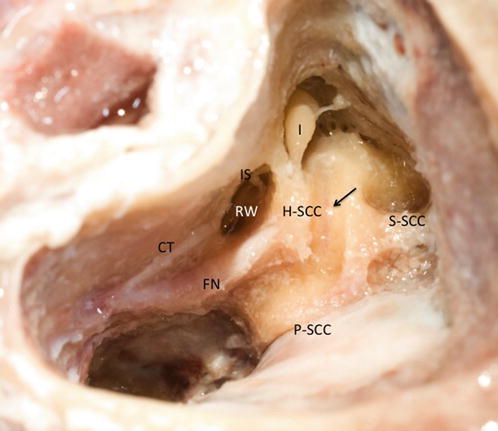
Fig. 11.1
Blue lining of the horizontal semicircular canal (H-SCC horizontal semicircular canal, arrow blue-lined H-SCC, S-SCC superior semicircular canal, P-SCC posterior semicircular canal, FN facial nerve, CT chorda tympani, RW round window, IS incudostapedial joint, I incus)
 The fenestrated canals (“snake eyes”) are followed in their extent to provide continuing landmarks
The fenestrated canals (“snake eyes”) are followed in their extent to provide continuing landmarks
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


