Keratoprosthesis Surgery
Claes H. Dohlman
Mahnaz Nouri
Why should we attempt to develop keratoprostheses (KPro) for corneal opacity when standard corneal transplantation is so well established and relatively safe? If the latter procedure were uniformly successful, there certainly would be no need for a KPro, with its even higher risks and greater demands on health resources. The answer lies in the stubborn failure rate of keratoplasty, in spite of a century of development. The outcome of keratoplasty varies markedly with underlying disease, geography, availability of donor tissue, health budget, and other factors, and it is still poorly documented. Some statistics are beginning to emerge, however, even if they are not population based but instead drawn from individual surgeons’ office practices—which automatically excludes the “inoperable” cases. For instance, the Eye Bank Association of America’s report for 2002 indicates that of a total of 33,000 transplants in the United States, more than 13% were done for failed grafts (1). (It is not known how many graft failures were not reoperated.) In a large outcome study, only 20% of regrafts for all causes remained clear for 5 years (2). In another group of first regrafts, again only 20% survived 5 years, whereas all repeat regrafts failed within the same time period (3). Moreover, on a world-wide basis, a large number of people with corneal blindness have no access to corneal surgery. The World Health Organization reports that approximately 6 million people are bilaterally blind from trachoma alone (4). Few of these patients receive a corneal transplant, and when it is performed, the failure rate is reportedly high.
The fact that standard keratoplasties have failed or have been deemed hopeless in such a large cohort of corneal patients does not automatically mean that a KPro is the immediate next step. In spite of efforts by fearless surgeons over 200 years, progress in developing long-lasting and safe KPro techniques has been slow. Creation of meaningful animal models has been difficult, and the long delay in the development of postoperative complications, many of them catastrophic, has made changes in technique and design slow in coming and hard to interpret. In spite of these impediments, however, very substantial progress has been made, especially during the past few decades. Rapid rehabilitation and sometimes spectacular vision in KPro eyes after corneal graft failures is now no longer a rarity. The long history of KPro development will not be detailed here—the reader is referred to earlier reviews (5,6).
The current KPro effort is maintained primarily in approximately a dozen centers worldwide and encompasses diverse approaches. One technique has been inspired by Strampelli (7), and a number of followers have modified the original principles further [Falcinelli et al. (8), Marchi et al. (9), Temprano (10), Grabner et al. (11), Liu et al. (12), Hille (13), and others]. This technique involves harvesting a tooth from the patient and preparing a slice of osteodental lamina to be used as a skirt for a cylinder of polymethylmethacrylate (PMMA), which is to be inserted (in two steps) into the patient’s cornea and covered by lid skin or buccal mucosal graft. The procedure is somewhat invasive but it has a reputation for stability and low rate of infection. Pintucci et al. (14), Girard et al. (15), Legeais et al. (16), and others have replaced the autologous tooth-derived skirt with “biocolonizable” porous plastic materials. In Russia, a large number of patients, especially with chemical burns, have been implanted with devices of different designs, but the optical core is still being made of PMMA (17,18). Yet another approach has been to develop a hydrogel sheet with porous edges to serve as an “artificial cornea.” It is implanted intrastromally and covered by a conjunctival flap. The center of the device is exposed later. This technique appears to be of value for graft failures in less inflamed eyes (19). Many smaller-scale efforts, some ingenious, are also currently under way (20).
In Boston, we have for a number of years used a PMMA KPro of a double-plated “collar button” design (21). Such a general configuration has been suggested in the past (22,23), and has been modified by us as described in the following section. Design and material of KPros are undoubtedly important in themselves, but it should be emphasized that the health of the surrounding tissue is vitally important. Without claiming superiority, we devote this chapter to the devices, surgical techniques, and follow-up routines that we have gradually developed.
DEVICES
The double-plated, or “collar button”-shaped devices we currently use come in two main designs (Fig. 66-1). The simple collar button (type I) is the most frequently used and is favored in eyes with reasonable blink and tear secretion mechanisms. Made of medical-grade PMMA, it consists of an anterior part with a 6-mm diameter front plate with an attached 3.35-mm stem with screw threads. A separate back plate is 7 mm in diameter and has eight holes, each 1.3 mm in diameter. The holes facilitate nutrition and hydration of the corneal graft, which is sandwiched between the two plates on completion (Fig. 66-1). Different modifications have been used in the past.
The type II device is similar except that it has a 2-mm long anterior nub designed to penetrate the skin or buccal mucosa in end-stage dry eyes (Fig. 66-1). The diameter of the front plate is now 6 mm. A posterior plate of 8.5-mm diameter is usually chosen. It has eight holes, each 1.5 mm in diameter.
The latest type I KPro has an anterior-posterior length of 3.7 mm and allows a maximum field of vision of 60 degrees. Type II is 4.7 mm long and can give a 40-degree field of vision. Details of the fabrication of these KPros have been described elsewhere (24).
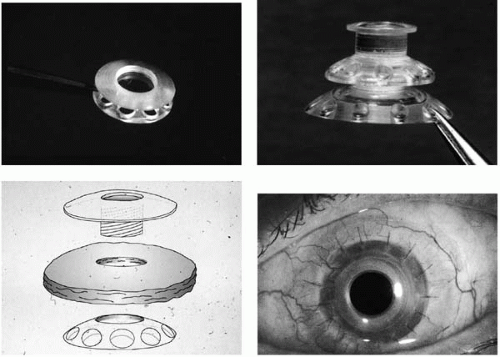 FIGURE 66-1. Upper left: The type I double-plated keratoprosthesis (KPro), the type most commonly used. It requires reasonably intact tear secretion and blink frequency. Upper right: The type II KPro, with a nub, is reserved for through-the-lid placement in end-stage dry eyes. Lower left: Principle of assembly of a type I KPro. A fresh corneal graft, with a punched 3-mm hole, is slid over the stem and the back plate is screwed on. The graft-KPro combination is then sutured in place like a standard corneal graft. The holes in the back plate facilitate nutrition and hydration of the overlying graft tissue. Lower right: Large-diameter soft contact lenses, worn indefinitely (with replacements), have proven highly protective of the corneal surface around the KPro. |
PROGNOSTIC CATEGORIES AND INDICATIONS
Analysis of our KPro results has clearly shown the detrimental role that inflammation, past and present, has on the long-term outcome. Severe inflammatory diseases carry a much worse prognosis for the KPro than after graft failures in noninflammatory conditions. This means that presumed autoimmune diseases such as pemphigoid, Stevens-Johnson syndrome, uveitis, and so forth, as well as past severe chemical burn, have a quite guarded prognosis. On the other hand, graft failures in relatively noninflammatory situations, such as when the initial condition was a corneal dystrophy or other edematous condition, or trauma, have good prognosis. Also, after infectious keratitis (bacterial, viral, fungal), long-term success is likely (25).
In more specific terms, we believe that a KPro type I is indicated in the nonautoimmune graft failure group, where blink and tear mechanisms are reasonably normal, and when visual acuity is less than 20/400. Also, the opposite eye should have suboptimal vision, such as 20/80 or less. When survival time is uncertain, old age strengthens this indication.
End-stage dry eyes (e.g., pemphigoid, Stevens-Johnson syndrome, some chemical burns) need a type II device,
which involves not only more complicated surgery, but a closer follow-up regimen and more frequent need for revision (26). The surgeon taking on this type of KPro surgery must be prepared to follow the patient for a lifetime.
which involves not only more complicated surgery, but a closer follow-up regimen and more frequent need for revision (26). The surgeon taking on this type of KPro surgery must be prepared to follow the patient for a lifetime.
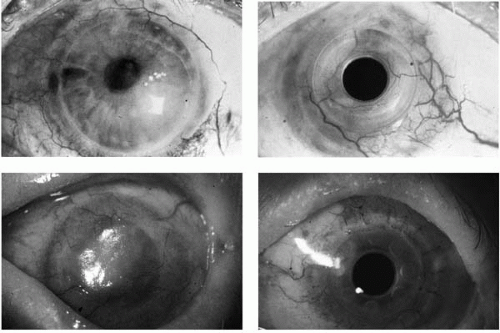 FIGURE 66-2. Upper left: Eye with repeated graft failures in lattice dystrophy. Upper right: Same patient as in upper left, 10 years after type I keratoprosthesis (KPro) insertion with a conjunctival flap. Vision is 20/20. Lower left: Long-standing Stevens-Johnson syndrome. Lower right: Same patient as in lower left; the KPro type I has been followed for 1 year and vision is 20/40. |
PATIENT EVALUATION
History
Documenting a detailed history of the ocular condition, as well as any important systemic disease, is mandatory. Duration of ocular symptoms (episodic, such as in herpes simplex, or steadily progressive), unilateral or bilateral, and status of the opposite eye should be explored in detail. Precise knowledge about previous surgery (e.g., cataract extraction, keratoplasty, glaucoma surgery, retina repair) is obviously crucial. A history of glaucoma is extremely important to solicit, especially after chemical burns, because the extent of optic nerve damage at the time of the examination is often very difficult to evaluate.
Visual Acuity
Standard refraction using a Snellen chart is usually sufficient to evaluate the degree of visual impairment. The next step, to ascribe relative contributions to the cornea, cataract, retina, or optic nerve disease, is not always easy in eyes that are so severely damaged that they are candidates for KPro. The corneal influence can be due to irregular surface or to stromal opacities, a question that can be solved by hard contact lens refraction. A visual field is rarely possible in these cases, but gross projection of a strong light source can be revealing. If nasal projection is absent and, particularly, if central fixation is uncertain, end-stage glaucoma with only finger-counting potential must be suspected.
Intraocular Pressure
Evaluation of the pressure in eyes with severely damaged cornea can be difficult and unreliable. The pneumotonometer is of more help than the applanation device, but both can give grossly erroneous readings. The phosphene tonometer is rarely of use when lids are thickened or when the visual field is restricted. Simple digital palpation gives only an approximate impression, but it is frequently the most reliable approach.
Blink Rate and Tear Secretion
Because evaporative damage to the corneal tissue around a KPro type I can be very detrimental, especially if a soft contact lens cannot be retained, tear film stability is very important. Therefore, poor blink rate and chronic exposure, as well as low tear secretion, must be taken into consideration. Blink rate and completeness should be noted before surgery when the patient does not feel he or she is being observed. Tear secretion should be evaluated with a standard Schirmer’s test. Quantifying breakup time is of little preoperative value.
Slit-Lamp Examination
This procedure is the cornerstone of the patient evaluation. The corneal surface should be judged for irregularity, keratinization, epithelial defects, and subepithelial vascularization. Stromal opacities, thickness, edema, and deep blood vessels should be evaluated separately, and drawings made. The lid structures should be inspected for lid surface incongruities, and the conjunctiva may show inflammation, important fornix shortening, or frank symblephara. Anterior chamber depth, appearance of pupil and iris, angle (narrow, closed?), the status of the lens or intraocular lens, all merit detailed notes in the record. The fundus is rarely seen well in KPro candidates, but an effort should be made to examine it with a 78- or 90-D lens and, if possible, the disk appearance recorded. Gross macular changes, such as massive age-related macular degeneration, may be observable. Indirect ophthalmoscopy of the peripheral retina should at least be attempted. During these maneuvers, special attention should be given to signs of inflammation, past or present, because of its importance for the prognosis of the contemplated KPro surgery.
Special Examinations
Ultrasonographic examination is necessary in most cases being evaluated for KPro. A retinal detachment must be ruled out with B-scan ultrasonography. This mode can also illuminate presence and degree of vitreous debris, but it cannot measure a glaucomatous optic nerve cupping with precision. Absence of a visible cup on the ultrasonogram does not guarantee a healthy nerve. If a glaucoma shunt has been previously implanted, a fluid cleft over the plate can usually be identified and, if present, it ensures patency of the intraocular tube. However, a visible cleft does not rule out existence of a dense capsule that has formed around the plate and which can obstruct flow enough to cause an unacceptably high intraocular pressure. Also, a B-scan can reveal the presence or absence of an intraocular lens. An A-scan measurement of the axial length of the eye is also mandatory to allow the selection of a KPro with the appropriate dioptric power. In our experience, electroretinography and visual evoked response are not of much value in KPro preoperative evaluation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


