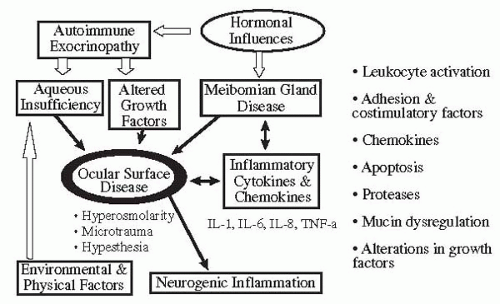
In spite of their rather diverse origins, the clinical presentation of patients with dry eye diseases is similar. Tear film instability is a component of all forms of dry eye disease, and tear hyperosmolarity is a key mechanism for the ocular surface damage. Aqueous-deficient dry eye is associated with reduced lacrimal function, but lacrimal function may be reduced as part of the aging process without producing the signs or symptoms of dry eye. The various factors to be considered in the diagnosis of KCS are (a) presence or absence of inflammation, (b) assessment of the function of lacrimal tissues, (c) determination of causes that could lead to decreased reflex tearing, (d) assessment of meibomian glands, and (e) environmental factors.
History
The patient’s history is extremely important in diagnosing dry-eye syndromes. Symptoms are a hallmark of the disease, and the most frequently encountered symptoms in patients with dry eyes are dryness, foreign-body or sandy sensation, burning, and photophobia. Patients may also complain of itching, excessive mucus secretions, heaviness of the eyelids, tight eyelids, inability to produce tears, pain, and redness. Moreover, as dry eye can coexist with other disorders (e.g., allergy), it is not unusual for patients to have symptoms due to multiple pathogenic mechanisms. The principal function of the tear film is to maintain a smooth, clear, refractive optical surface in a hostile external environment. Any adverse effect on the corneal regularity and clarity will interfere with vision and may cause symptoms. Patients often use the term “dryness” to describe their condition but will have difficulty defining exactly what this means. The term “discomfort” may be a more accurate summation of all the patient’s symptoms. Various questionnaires have been developed (
72,
73,
74) to assess symptoms in dry eye patients. These questionnaires
are useful tools for clinical treatment trials in dry eye patients.
Dry eye patients are exquisitely sensitive to drafts and winds. Often they volunteer information regarding their intolerance to air conditioning or driving in the car with the windows down. Patients with KCS feel worse in a dry, cold environment and under conditions of increased evaporation. Reading is often difficult for dry eye sufferers. This probably occurs because the blink frequency decreases during tasks requiring concentration. Patients often complain that nighttime or awakening is the worst part of their day. Sleep (like general anesthesia) decreases tear production. If the eye is already compromised with regard to tear flow, further reduction during sleep may be enough to produce nocturnal symptoms. This is especially true if concurrent blepharitis or lagophthalmos is present. Smoke is almost universally intolerable to tear-deficient patients. Because smoke is actually a suspension of solids in air, the particulate bombardment of the ocular surface produces discomfort. Determining whether symptoms are worse or better indoors or out, at work or at home, will aid in identifying environments that need to be modified to improve the patient’s symptoms.
Patients should be asked whether they are able to produce irritant and emotional tears. “Do you get tears when you peel onions? Can you cry when you feel sad or hurt? Affirmative responses suggest some lacrimal gland function remains, whereas negative answers suggest that the lacrimal gland is incapable of secreting tear fluid in response to any stimuli. In patients with KCS, the ability to generate irritant tears is lost before the ability to generate emotional tears.
“What medications do you take?” should also be asked. Systemic antihistaminics, antidepressants, anticholinergics, and diuretics are most responsible for decreased tear production. The use of systemic steroids and other immunosuppressives, such as hydroxychloroquine (Plaquenil), methotrexate, and cyclophosphamide (Cytoxan), which may be used in treating patients with Sjögren’s syndrome and other collagen vascular diseases should be noted.
It is important to determine whether the patient has any associated systemic symptoms or diseases. Important questions should be directed toward detecting a history of dry mouth (xerostomia) or dental and gum disease. Patients with Sjögren’s syndrome and xerostomia are at greater risk of dental and gum disease owing to lack of saliva. Questions that help in determining whether the patient has significant xerostomia include the following: “Can you feel saliva in your mouth?” “Can you swallow bread or meat without additional fluids?” Women should be asked whether they have experienced a noticeable decrease of vaginal secretions. Patients should be asked if they have ever been told they have Sjögren’s syndrome, lupus, rheumatoid arthritis, systemic sclerosis, vasculitis, thyroid disease, lymphoma, or AIDS. If the patient has had a Bone Marrow Transplant, a history of rejection or graft-versus-host disease should be noted.
“Do you have any skin problems?” is a question that should always be asked. Although primary dermatologic illness is rarely the cause of dry eye, looking for such illnesses often provides useful clues. Examples are numerous: scleroderma, scurvy, thrombotic thrombocytopenic purpura, the facial rash in lupus (all these are seen in association with Sjögren’s syndrome), skin lesions in pemphigoid, old scars from Stevens-Johnson syndrome, and acne rosacea (associated with lipid abnormalities). An equally important reason for exploring skin problems during history taking is to discover entities that may mimic tear deficiency. Many skin disorders are associated with superficial punctate keratopathy and may present a picture that could be confused with sicca. Some of these are seborrheic dermatitis, psoriasis, ichthyosis, and keratosis follicularis (Darier’s disease). Family history should be elicited as to whether there is any blood relative with KCS, Sjögren’s syndrome, collagen vascular disease, and other eye diseases.
Information should be obtained regarding use of lubricants and medications, including drops as well as ointments. Inquire about these specifically, as most patients will not consider topical treatment when asked generally about medications. “Are the topical lubricants preserved or unpreserved?” “How long have they been used and how often?” Most patients with KCS improve with topical lubricant therapy. The severity of a patient’s KCS often can be determined by how frequently topical lubricants are used. Patients with severe KCS use topical lubricants more frequently than those with mild KCS. It is also important to remember that patients with moderate to severe KCS can be made worse by topical lubricants containing preservatives. Furthermore, any topical medication is potentially toxic due to the patient’s inability to dilute it because of a lack of aqueous tear secretion. Patients should be asked whether they have had previous placement of temporary collagen plugs or silicone plugs, or whether previous permanent occlusion with laser or cautery has been performed. If so, then one should ask whether there was an improvement in symptoms and whether epiphora occurred.