Juvenile nasopharyngeal angiofibromas (JNAs) are rare, benign, highly vascular, locally aggressive tumors that primarily affect male adolescents. Historical treatment of these neoplasms has been primarily surgical. In the past decade, endoscopic resection of JNAs has become a viable and promising surgical treatment option. Endoscopic resection has many advantages over traditional open techniques, including better cosmesis, decreased blood loss, shortened hospital stays, and equivalent or improved recurrence rates. Emerging endoscopic technology continues to push the boundaries of resection of skull base tumors and will no doubt become the surgical treatment of choice for most JNAs in the near future.
| EBM Question | Level of Evidence | Grade of Recommendation |
|---|---|---|
| Is morbidity less with endoscopic resection (blood loss, cosmesis, CN injury, etc) compared to open surgery? | 3b | C |
- •
Endoscopic resection of early-stage juvenile nasopharyngeal angiofibromas (JNAs) is a safe and surgically sound treatment that has multiple advantages over traditional open approaches, including better cosmesis, decreased blood loss, shortened hospital stay, and equivalent or improved recurrence rates.
- •
Magnetic resonance imaging (MRI) is the imaging standard for postoperative surveillance and should be performed within the first postoperative year to detect recurrent/residual disease.
- •
First described by Chaveau in 1906, JNAs are highly vascular benign tumors that primarily affect the young male population. These neoplasms are rare, accounting for approximately 0.05% of head and neck tumors. Although benign and slow growing, these tumors are locally aggressive and can cause extensive bone destruction, intracranial hemorrhage, facial deformity, severe epistaxis, and blindness. JNAs derive from the superior border of the sphenopalatine foramen. As the tumors enlarge, they extend through well-defined pathways into the infratemporal fossa, cavernous sinus, sphenoid sinus, middle cranial fossa, and, rarely, anterior cranial fossa. Surgical resection has been the mainstay of treatment of JNAs, and multiple open surgical approaches have been proposed depending on the location and extent of the tumor. Radiation therapy has been mostly reserved for unresectable tumors, residual disease after surgical resection, or recurrences occurring in anatomically critical areas. However, over the past 2 decades, endoscopic techniques and technology have improved, and an increasing number of JNAs are being removed endoscopically or in combination with traditional open approaches. Endoscopic techniques offer many advantages over open approaches, with better cosmesis (no external surgical scar), reduced intraoperative blood loss (usually combined with preoperative embolization), decreased hospital stays, and improved or equivalent recurrence rates.
Symptoms of JNA
The most common presenting symptoms of patients with JNA are unilateral nasal obstruction occurring in 91% and epistaxis occurring in 63% of patients. Other related symptoms include nasal discharge; pain; sinusitis; facial deformity; otologic symptoms, such as hearing impairment and otitis media; and ocular symptoms of proptosis and diplopia. Symptoms are generally present for 6 months to a year before the patient is diagnosed. JNAs are typically found in the male population between the ages of 10 and 24 years, with a median age at diagnosis of 15 years.
Pathology of JNA
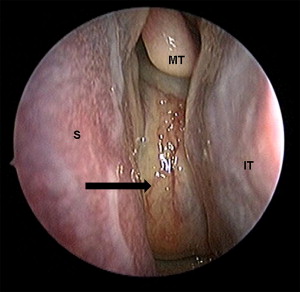
JNAs are characterized on gross pathology as well-defined, mucosalized, red to purple masses found in the nasal cavity and nasopharynx ( Fig. 1 ). Histologically, the tumor is composed of 2 main components: spindle- or stellate-shaped cells embedded in a rich collagen matrix and a complex vascular arrangement of blood vessels that vary in size from capillaries to large venous channels. Characteristically, these vessels lack elastic laminae and elastic fibers and have vascular walls that vary in thickness. These features account for the tendency of these tumors to hemorrhage easily. JNAs occur exclusively in men and are thought to be partially androgen dependent. JNAs possess multiple hormone receptors, including testosterone, dihydrotestosterone, and androgen. However, investigation into hormone therapy for these tumors has been disappointing. JNAs may originate from a residual vascular plexus left behind after the involution of the first branchial artery, but the cause of JNAs is still under debate.
Pathology of JNA
JNAs are characterized on gross pathology as well-defined, mucosalized, red to purple masses found in the nasal cavity and nasopharynx ( Fig. 1 ). Histologically, the tumor is composed of 2 main components: spindle- or stellate-shaped cells embedded in a rich collagen matrix and a complex vascular arrangement of blood vessels that vary in size from capillaries to large venous channels. Characteristically, these vessels lack elastic laminae and elastic fibers and have vascular walls that vary in thickness. These features account for the tendency of these tumors to hemorrhage easily. JNAs occur exclusively in men and are thought to be partially androgen dependent. JNAs possess multiple hormone receptors, including testosterone, dihydrotestosterone, and androgen. However, investigation into hormone therapy for these tumors has been disappointing. JNAs may originate from a residual vascular plexus left behind after the involution of the first branchial artery, but the cause of JNAs is still under debate.
Imaging
Computed tomography (CT) and MRI are both critical to the proper evaluation of angiofibromas. CT better delineates bony details of the skull base, including bony erosion, in particular, the depth of invasion into the bone of the sphenoid sinus, a main predictor of recurrence ( Fig. 2 ). The extent of invasion into the cancellous bone of the sphenoid is difficult to determine intraoperatively, and this leads to a high likelihood of residual tumor and recurrence. CT scans are also commonly used for intraoperative stereotactic surgical navigation systems to confirm the extent and resection of tumor. On the other hand, MRI is crucial for highlighting soft tissue elements of the tumor and assesses the relation of the tumor to critical structures such as the internal carotid artery, cavernous sinus, and pituitary gland ( Fig. 3 ). Recurrence and residual tumors are best appreciated on MRI.
The pathognomonic radiologic feature of JNAs is the anterior bowing of the posterior maxillary wall, termed the Holman-Miller sign. Other radiologic features include a mass originating at the sphenopalatine foramen and erosion of the mass into the pterygomaxillary fossa, sphenoid sinus, and infratemporal fossa.
Further confirmation of the JNA diagnosis is usually provided by angiography, which also doubles as treatment with embolization. Angiography provides information on the specific blood supply of the tumor. Distal branches of the internal maxillary artery, a branch of the external carotid, provide the major blood supply for most JNAs, but, as tumors grow, they may also develop vascular supply from branches of the ipsilateral internal carotid artery and contralateral external carotid artery. Fig. 4 shows the extensive vascular network of a JNA as seen in reconstructed images from angiography and CT angiography.
Staging for nasopharyngeal angiofibromas
Several staging systems for nasopharyngeal angiofibromas have been proposed, all based on extension of the tumor. The 3 most prevalent staging systems are those of Andrews’ (modified Fisch), Chandler’s, and Radkowski’s (modification of Sessions’ classification). JNAs are classified depending on the extension of tumor and amount of intracranial extension. At present, there is no single universally adopted classification system. To better interpret the results of this article, all 3 classification systems have been included in Tables 1–3 . A recently proposed endoscopic staging system for angiofibromas by Snyderman and colleagues focuses on residual vascularity (after preoperative embolization) and route of intracranial extension. This novel classification aims to better predict morbidity and prognosis by focusing on these 2 critical features.
| Stage | Description |
|---|---|
| I | Tumor limited to the nasal cavity and nasopharynx |
| II | Tumor extension into the pterygopalatine fossa, maxillary, sphenoid, or ethmoid sinuses |
| IIIa | Extension into orbit or infratemporal fossa without intracranial extension |
| IIIb | Stage IIIa with small extradural intracranial (parasellar) involvement |
| IVa | Large extradural intracranial or intradural extension |
| IVb | Extension into cavernous sinus, pituitary, or optic chiasm |
| Stage | Description |
|---|---|
| I | Confined to nasopharynx |
| II | Extends into nasal cavity and/or sphenoid |
| III | Extends to 1 or several of the following: antrum, ethmoids, pterygomaxillary and infratemporal fossa, orbit, and/or cheek |
| IV | Extends into cranial cavity |
| Stage | Description |
|---|---|
| IA | Limited to nose and nasopharyngeal area |
| IB | Extension into 1 or more sinuses |
| IIA | Minimal extension into pterygopalatine fossa |
| IIB | Occupation of the pterygopalatine fossa with or without orbital erosion |
| IIC | Infratemporal fossa extension with or without cheek or pterygoid plate involvement |
| IIIA | Erosion of the skull base (middle cranial fossa or pterygoids) |
| IIIB | Erosion of skull base with intracranial extension with or without cavernous sinus involvement |
Treatment options for JNA
Surgical resection is widely accepted as the treatment modality of choice for JNAs. Multiple surgical approaches have been proposed and are often based on tumor size, location, and extent. Recently, endoscopic approaches have been adopted, secondary to the likelihood of decreased morbidity. Adjunctive radiation, hormone therapy, and chemotherapy have all been explored, with hormone therapy and chemotherapy nearly abandoned because of ineffectiveness and significant side effects. However, radiation therapy is still widely used, although primarily saved for advanced tumors that would have a high morbidity with attempted resection or residual/recurrent disease in critical anatomic areas. To complicate the issue of treatment, JNAs may spontaneously regress without any treatment once the patient completes adolescence. Spontaneous involution has been documented in multiple case reports.
Radiation Therapy for JNA
Recent studies using radiation therapy as the definitive treatment of advanced JNAs have shown impressive local control rates of 85% to 91%. Reddy and colleagues treated 15 patients with Chandler stage III or IV disease with 30 to 36 Gy of radiation, with a local control rate of 85%. Two patients with continued growth required further treatment with surgical salvage. The investigators also noted that tumor regression could take up to 2 years or more. An extension of this study treated 7 additional patients (reporting as a total of 22) and claimed a local control rate of 91% with no severe complications. Lee and colleagues treated 27 patients with 30 to 40 Gy, with 4 patients (15%) ultimately developing further growth requiring additional treatment. In the rest (85%), the tumor remained stable in size or regressed. However, the investigators did not consider radiographic abnormalities on imaging as residual or recurrent disease. Only if the patient became symptomatic or new radiographic findings developed was the condition considered to have recurred. Although rare, radiation may lead to devastating sequelae, including secondary head and neck malignancies, in this young population. Reddy and colleagues had 1 patient who develop a basal cell carcinoma of the skin. Malignant transformation of the tumor with increasing radiation doses has also occurred in a small number of cases. Other complications of radiation therapy include panhypopituitarism, growth retardation, cataracts, radiation keratopathy, temporal lobe necrosis, and delayed transient central nervous system syndrome. Newer radiation techniques, such as intensity-modulated radiation therapy, may provide the same local control rates with less morbidity but are still under investigation for the treatment of JNAs.
Embolization
Before a debate on surgical techniques can begin, the issue of preoperative embolization must be introduced. It is well accepted that preoperative embolization of JNAs significantly decreases blood loss during resection and improves visualization for more complete tumor removal. Li and colleagues found that operative blood loss in patients who underwent embolization was approximately half compared with those who did not undergo embolization (677 mL compared with 1136 mL). In addition, in patients who did have a transfusion, those who underwent embolization required only 400 mL of blood, whereas those who did not undergo embolization required 836 mL (a reduction of 50%). However, the significant risks of embolization cannot be discounted. These risks include, but are not limited to, neurologic deficits (numbness, facial paralysis), stroke, and blindness. Herman and colleagues recently published a novel embolization technique with Onyx, a liquid embolic agent that is directly injected into the tumor under fluoroscopic and endoscopic guidance, that may prove to be safer and less invasive than traditional techniques. Some investigators propose that preoperative embolization distorts tumor boundaries, leading to incomplete resection, especially if the tumor extends into the basisphenoid. Lloyd and Mann and colleagues both suggest that preoperative embolization may increase recurrence rates secondary to incomplete tumor removal. Techniques to decrease bleeding without preoperative embolization have included hypotensive general anesthesia, with some reporting excellent results. With novel technologies, such as radiofrequency coblation, tumors may be resected with significantly less blood loss, and preoperative embolization may ultimately be deemed unnecessary for lower-stage tumors. For example, Ruiz has routinely used coblation for the resection of JNAs without preoperative embolization. Overall, however, in most endoscopic series, patients still undergo preoperative embolization 24 to 48 hours before surgery (significant contributions may develop from contralateral vessels several days after embolization).
Open Surgical Treatment of JNA
Multiple surgical approaches have been used for the resection of JNAs, including transpalatal, lateral rhinotomy, midface degloving, medial maxillectomy, transantral, infratemporal fossa, and frontotemporal craniotomy. Different investigators recommend varied approaches, all dependent on the location and extension of the tumor. Before endoscopic approaches, the transpalatal and midface degloving approaches were popularized because they require no external surgical incisions. Howard and colleagues treated 19 cases of JNA with the midface degloving approach and reported no recurrences with 6 months to 3 years of follow-up. Tyagi and colleagues used an extended transpalatal/transmaxillary approach for stage IIIa and IIIb disease (Andrews’ classification) in 75 patients with a recurrence rate of 13%. The most common surgical complications were secretory otitis media and palatal fistulas. Hosseini and colleagues used a transpalatal approach in 27 of 37 patients ranging from stage Ia to stage IIIb disease (Radkowski’s classification), with 2 having residual disease and 4 patients developing recurrence. The most common postoperative complication was oronasal fistula.
Endoscopic Resection
Endoscopic resection of benign and malignant neoplasms has gained significant ground in the past decade as a valuable alternative surgical approach. Endoscopic surgery has advantages over traditional open approaches, specifically in the male adolescent population that is affected by JNA. Endoscopic resection avoids osteotomies, which have been implicated in inhibiting facial growth. This technique also requires no external incision or facial deforming scar, a concern in a population that is just beginning to develop their self-perception. In addition, endoscopes offer magnification and angled views for excellent tumor visualization not provided by open approaches. Many investigators have detailed the feasibility of endoscopic approaches to early-stage JNAs. However, controversy has abounded over which JNAs are most appropriate for endoscopic removal. Most investigators concede that early-stage JNAs (stage I, II, and some stage III) can be adequately removed endoscopically ( Figs. 5 and 6 ). Proponents of endoscopic resection report decreased length of hospital stays, reduced intraoperative blood loss, and equivalent or reduced recurrence rates compared with open approaches.



