This article presents a detailed case report of a patient who was diagnosed with superior canal dehiscence at 37 years of age, but who had a suspicious history for that syndrome from at least 10 years of age. The authors hypothesize several reasons for this late diagnosis, with the goal of helping pediatricians, otolaryngologists, and neurologists consider this syndrome in their differential diagnosis of children, adolescents, or adults experiencing dizziness.
Superior canal dehiscence syndrome was first described by Minor and colleagues in 1998. Typical symptoms include hyperacusis for bone-conducted sounds with autophony, and vertigo induced by loud sounds (Tullio phenomenon) or increased pressure in the middle ear (Hennebert sign) or intracranial space (eg, during strenuous activities).
The pathophysiology of the dehiscent bone over the superior semicircular canal is still debated. Symptoms and signs of semicircular canal dehiscence syndrome (SCDS) typically occur in adulthood. Nevertheless, a developmental or congenital anomaly is suspected because thinning of the bone overlying the superior canal often occurs bilaterally, as shown in CT and temporal bone dissection studies. This thin bone could then presumably be disrupted by trauma or erosion caused by pressure of the overlying temporal lobe. A genetic defect has not yet been identified (Gürtler N, personal communication, 2009). Thin bone overlying the superior semicircular canal on the side contralateral to a dehiscence has been reported both on CT scans and in temporal bones. However, a long-term study with follow-up CT or vestibular evoked myogenic potentials (VEMPs) to assess the development of SCD on the intact side has not been reported. One case report of a 7-year-old girl with SCD on the right and one recent report of a 4-year-old child with a partial dehiscence of the right posterior semicircular canal have been published. Otherwise, SCDS in children seems to be rare, underdiagnosed, or not published.
A defect in the bone overlying the superior semicircular canal can also be caused by trauma (although the force needed to create a defect is unknown, and whether a thinning of the bone must exist before the trauma occurs is also unclear), cholesteatoma, vestibular schwannoma, meningioma, or even glioblastoma, but these are rarely found with SCDS, so one or more other causes seem more likely in most cases. No evidence currently supports the theory of osteoporosis as a potential cause of semicircular canal dehiscence. The authors still believe that a developmental defect is the most likely cause for SCDS, especially because the bone overlying the SC is the last part of the temporal bone to form in development. Nevertheless, why the diagnosis is usually first made in adulthood remains an enigma.
This article presents a case report of patient who was diagnosed with SCDS at 37 years of age, whose typical symptoms had begun in the classical form approximately 3 years earlier. However, a detailed and specific history revealed that some symptoms had already begun at approximately 10 years of age.
Case report
A 37-year-old man was seen in the authors’ interdisciplinary center for vertigo and balance disorders in 2005. He complained of periods of dizziness that were usually provoked by loud sounds, especially when he had to speak loudly in conferences or in restaurants with a noisy background. He never experienced true rotatory vertigo. These spells of dizziness increased at 34 years of age, after which his sensitivity to noise also increased, to the point where he could even hear his own eye movements in his right ear and other sounds produced by his own body, such as footsteps and his own voice. Dizziness increased with exertion in sport activities until he could not even jog after 35 years of age.
Physical examination showed normal outer ear canals and eardrums with normal Eustachian tube function, but during Valsalva maneuver he felt a slight shift of the visual scene and dizziness. The Weber tuning fork test lateralized to the right ear, and the Rinne test was positive bilaterally. Hennebert’s sign was positive, so that both positive and negative pressure in the right outer ear canal provoked a shifting of the visual scene. When repeating these signs under Frenzel goggles, the authors noted small torsional movements of the eyes toward the left side while positive pressure was applied, which reversed when negative pressure was applied. Vertical and horizontal components could not be seen. This simple investigation alone was sufficient for SCDS to be suspected.
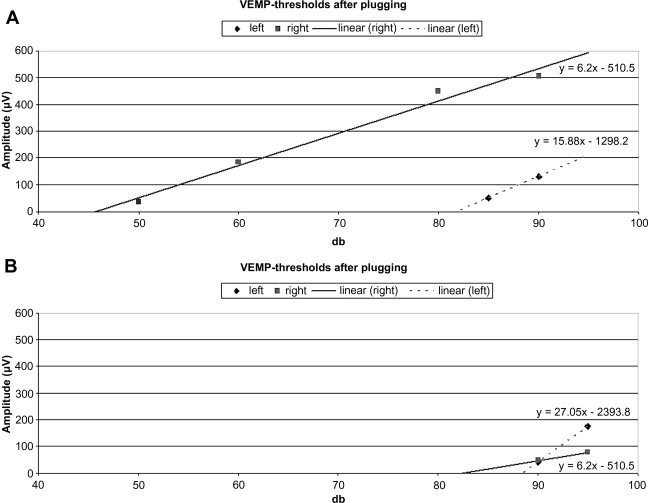
Audiometry supported the clinically suspected air–bone gap at least at 500 Hz, and cervical VEMPs in response to acoustic clicks confirmed a reduced threshold of approximately 46 dB nHL on the right and a normal threshold (82 dB nHL) on the left ( Fig. 1 A). CT of the temporal bones showed dehiscence of the right superior semicircular canal ( Fig. 2 A).

In a more detailed history, the authors found that even beginning at approximately 10 years of age, the patient experienced periodic vague dizziness, especially in train stations, shopping centers, and other noisy public places. His symptoms increased with exertion in sporting activities, especially when riding his bicycle uphill. He felt best in quiet environments and when lying in bed. He avoided common social activities with friends, and later also with colleagues, because he found them too noisy; he preferred quiet. He often told his parents that something must be wrong, and was evaluated by several physicians who considered diagnoses such as vitamin deficiencies and even psychogenic causes. Before presenting to the authors’ clinics, the conclusion was simply that he had to live with these symptoms.
The authors saw no indications of panic disorder, depression, or any other psychogenic disturbances. The patient had a good sense of humor, was intelligent and insightful, and was running his own company successfully in a very competitive field. No indication was seen that he was somatizing or overestimating his symptoms. After he learned the diagnosis and the operative treatment option, he chose to wait 3 more years, during which time the symptoms became even stronger and, ultimately, intolerable, at which point he decided to pursue surgical treatment.
The dehiscent canal was plugged using the middle cranial fossa approach without complications. In the immediate postoperative period, air conduction thresholds were almost identical to the preoperative audiogram. Bone conduction thresholds were still slightly better than air-conduction thresholds. In absolute silence he was still able to hear his eyes moving with his right ear, but markedly less so than preoperatively, and it was not bothersome. Vestibular function was reduced only for the plugged superior canal, because he showed evidence of a deficient vestibuloocular reflex for rapid head thrusts exciting the plugged canal but none of the other canals on the ipsilateral side.
Within 48 hours of surgery the patient noted profound changes, even commenting on what seemed like a “new life.” First, he noted that he no longer heard his voice, eye movements, or other body sounds in the affected ear. Second, he noted that ambulation, particularly outdoors, felt more stable. Finally, he found that ambient noise no longer seemed to disturb his equilibrium or sense of well-being. Reflecting on this, he commented that only after surgery did he realize how often since childhood he had altered his routine or environment to avoid noisy situations and the associated disequilibrium. He now enjoys going to social events and restaurants, and has been able to resume sporting activities without feeling dizzy. Loud sounds no longer disturb him, and he has no fear of crowds or busy places.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


