Ménière’s disease (MD) is characterized by episodic vertigo, fluctuating hearing loss and tinnitus, and by the presence of endolymphatic hydrops on postmortem examination. This disease continues to be a diagnostic and therapeutic challenge. Patients with MD range from minimally symptomatic, highly functional individuals to severely affected, disabled patients. Current management strategies are designed to control the acute and recurrent vestibulopathy but offer minimal remedy for the progressive cochlear dysfunction. Recent research highlights the role of neurotoxicity in the pathogenesis of the cochleovestibular deterioration. This article discusses a patient with MD, and provides an algorithm for the management of this disease.
Ménière’s disease (MD) is characterized by episodic vertigo, fluctuating hearing loss, aural pressure, and tinnitus. Since its description by Prosper Ménière’s in the Gazette Médicale de Paris in 1861, the pathophysiology and management of MD has been a controversial topic. Depending on the geographic location, the incidence of MD varies between 4.3 and 15.3 per 100,000. Affected individuals are usually between the fourth and sixth decades of life, with a female/male ratio of 1.3:1.
The Committee on Hearing and Equilibrium of the American Academy of Otolaryngology-Head and Neck Surgery published the defining guidelines of Ménière’s disease ( Table 1 ). Based on the residual hearing and residual vertigo after treatment, staging systems and classification schemes have been proposed ( Tables 2 and 3 ).
| Definition | Symptoms |
|---|---|
| Certain Ménière’s disease | Definite Ménière’s disease plus histopathologic confirmation |
| Definite Ménière’s disease | ≥2 definitive spontaneous episodes of vertigo 20 min or longer Audiometrically documented hearing loss on at least 1 occasion Tinnitus or aural fullness in the treated ear Other causes excluded |
| Probable Ménière’s disease | One definitive episode of vertigo Audiometrically documented hearing loss on at least 1 occasion Tinnitus or aural fullness in the treated ear Other causes excluded |
| Possible Ménière’s disease | Episodic vertigo without documented hearing loss, or Sensorineural hearing loss fluctuating or fixed, with dysequilibrium but nonepisodic Other causes excluded |
| Stage | Four-tone Average (dB) |
|---|---|
| 1 | ≤25 |
| 2 | 26–40 |
| 3 | 41–70 |
| 4 | >70 |
| Numerical Value | Class |
|---|---|
| 0 | A |
| 1–40 | B |
| 41–80 | C |
| 81–120 | D |
| >120 | E |
| Secondary treatment initiated because of disability from vertigo | F |
The diagnosis of MD, an idiopathic condition, is made after excluding other causes that may mimic the disorder. Several pathologic conditions can masquerade as MD and are best referred to as Ménière’s syndrome. These conditions can be infectious (otosyphilis), autoimmune (Cogan syndrome, autoimmune inner ear disease), and neoplastic (eg, intralabyrinthine or vestibular schwannomas, endolymphatic sac tumors).
This article presents a clinical vignette of a patient with MD who ultimately displays the full spectrum of the disease, and discusses the clinical presentation, the diagnostic evaluation, and the different therapeutic modalities. The article provides the essential points that can help guide the assessment and management of this condition.
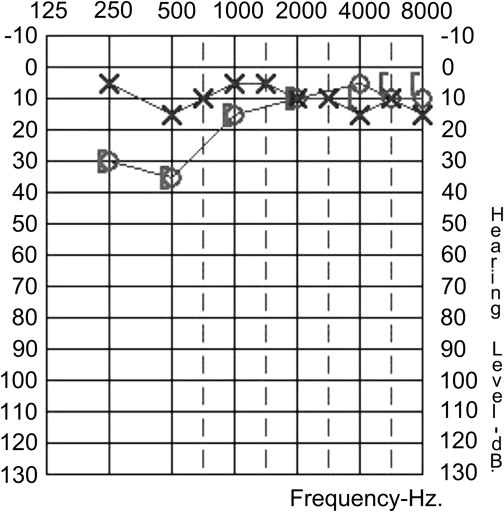
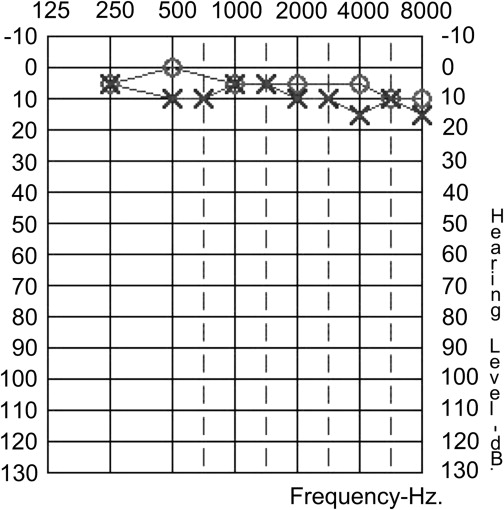
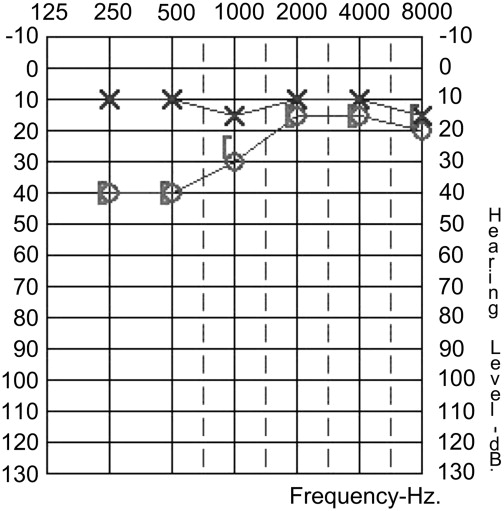
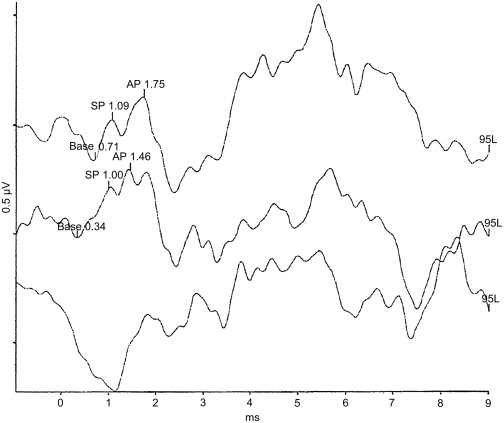
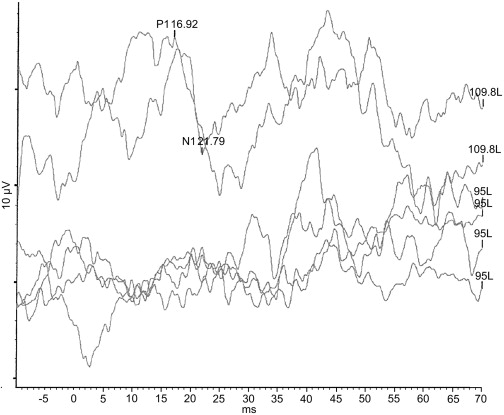
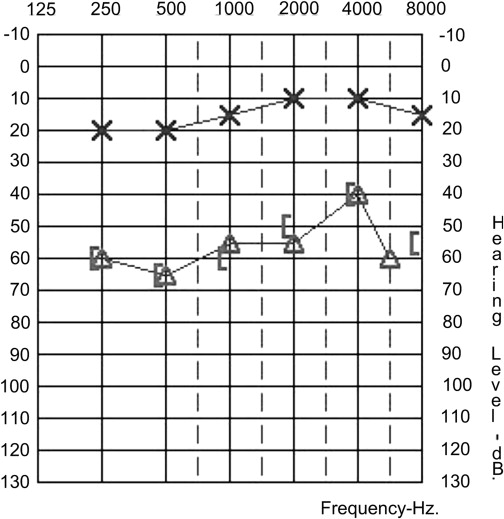
A.S. is a 34-year-old woman, healthy without any significant past medical history, who presented to the otology clinic 10 years ago for evaluation of a 3-day complaint of a right- sided muffled hearing, sensation of ipsilateral aural fullness and a low-pitched oceanlike sound. She denied vertigo or significant disequilibrium. She denied any recent viral illnesses. The otoscopic examination was normal. She had a similar episode 8 months earlier, which spontaneously resolved. An audiogram performed at that time is shown in Fig. 1 , which reveals a right-sided, low-frequency rising to normal sensorineural hearing loss with excellent word discrimination score (WDS). Her tympanogram and stapedial reflexes (not shown) were normal. A follow-up audiogram, performed 3 weeks following the initial presentation ( Fig. 2 ), showed normal hearing thresholds. A repeat audiogram was performed during the current visit ( Fig. 3 ) and revealed a moderate rising to mild, low-frequency sensorineural hearing loss. The WDS was 84%. The Stenger test was negative. A gadolinium-enhanced magnetic resonance imaging (gado-MRI) study, centered on the internal auditory canals, was normal. An electrocochleography showed an increased summating potential (SP)/action potential (AP) ratio at 0.64:0.74 microvolts on the right side ( Fig. 4 ), with the contralateral ear showing a normal ratio less than 0.4 (not shown). The presumed diagnosis was cochlear hydrops (CH). She completed a 10-day course of prednisone, and instructions were given for a low-salt diet. Her hearing returned to normal. Six months later the patient developed recurrence of her right-sided hearing loss, aural fullness, roaring right-sided tinnitus, and a vertigo spell that lasted approximately 3 hours and was associated with nausea and vomiting. She also described a subjective sensation of falling backward. On examination, she had a right-beating horizonatal nystagmus, which increased in amplitude on right lateral gaze. A vestibular evoked myogenic potential (VEMP) showed an increased threshold on the left side ( Fig. 5 ). The audiogram showed a moderate rising to mild sensorineural hearing loss ( Fig. 6 ). The WDS was 76%. She was treated with a course of steroids and started on hydrochlorothiazide and triamterene. The patient’s symptoms were consistent with the diagnosis of right-sided probable MD.
What is CH? What is its significance?
The term CH has been used to describe fluctuating hearing loss without associated vertigo, which may represent an earlier phase of a continuum, ranging from mild cochlear involvement to full cochleovestibular dysfunction as seen in MD.
House and colleagues studied the relationship between CH and MD. In their retrospective review of 950 hydropic ears, 71% were diagnosed with unilateral MD and 29% were labeled as unilateral CH. Bilateral MD at presentation was seen in 11%, with another 14% of unilateral MD becoming bilateral MD. Of patients initially diagnosed as having unilateral CH, 33% developed MD during an average of 7.6 years of follow-up.
What is the pathophysiology of CH and Ménière’s disease?
Although endolymphatic hydrops (ELH) is felt to be the underlying histopathologic correlate in MD, to date no histopathologic study has confirmed the presence of ELH in patients with CH. Despite the lack of direct evidence of this association, electrophysiologic studies showing increased SP/AP ratios suggest the presence of ELH.
The pathophysiology of hydrops remains unknown. Several intrinsic (genetic, anatomic, autoimmune, or vascular) or extrinsic (allergic, viral, or trauma) factors can cause disturbance in the mechanisms involved in the regulation of endolymphatic fluid homeostasis. Whether this disturbance causes a predominant alteration in the longitudinal versus radial flow of endolymph has long been debated. However, it remains unclear whether the produced hydrops is the result of cytochemical abnormality or anatomic anomaly.
The sine qua non relationship of ELH to the symptoms of MD has also been questioned as to whether the observed ELH is the direct pathologic initiator of cochleovestibular dysfunction or is an epiphenomenon of a subtler biochemical perturbation. In a review of their temporal bone registry, Merchant and colleagues found that all 28 patients with Ménière’s syndrome had evidence of ELH. However, of the 79 patients with ELH, only 51 had Ménière’s symptoms. Classic symptoms were absent in 9 of 35 patients with idiopathic hydrops and in 42 of 44 patients with secondary hydrops.
What is the pathophysiology of CH and Ménière’s disease?
Although endolymphatic hydrops (ELH) is felt to be the underlying histopathologic correlate in MD, to date no histopathologic study has confirmed the presence of ELH in patients with CH. Despite the lack of direct evidence of this association, electrophysiologic studies showing increased SP/AP ratios suggest the presence of ELH.
The pathophysiology of hydrops remains unknown. Several intrinsic (genetic, anatomic, autoimmune, or vascular) or extrinsic (allergic, viral, or trauma) factors can cause disturbance in the mechanisms involved in the regulation of endolymphatic fluid homeostasis. Whether this disturbance causes a predominant alteration in the longitudinal versus radial flow of endolymph has long been debated. However, it remains unclear whether the produced hydrops is the result of cytochemical abnormality or anatomic anomaly.
The sine qua non relationship of ELH to the symptoms of MD has also been questioned as to whether the observed ELH is the direct pathologic initiator of cochleovestibular dysfunction or is an epiphenomenon of a subtler biochemical perturbation. In a review of their temporal bone registry, Merchant and colleagues found that all 28 patients with Ménière’s syndrome had evidence of ELH. However, of the 79 patients with ELH, only 51 had Ménière’s symptoms. Classic symptoms were absent in 9 of 35 patients with idiopathic hydrops and in 42 of 44 patients with secondary hydrops.
What is the role of adjunctive tests in the diagnosis of MD?
A national survey showed that, depending on the region (west, midwest, northeast, New England, and Atlantic coast), 26.9% to 46.7% of treating otolaryngologists relied on history, physical examination, and audiometry alone to establish the diagnosis of MD. Others obtained adjunctive tests to support their diagnosis.
Electrophysiologic Studies
In recent years, several diagnostic tests have been proposed to study the presence of ELH and complement the diagnosis of CH or MD. Two electrophysiologic tests merit discussion: electrocochleography (ECoG) and VEMPs.
Electrocochleography is an evoked potential in response to condensation and rarefaction click or tone burst stimuli recorded by an intratympanic or extratympanic electrode. The SP and AP of the eighth nerve are recorded. An increased SP/AP ratio (greater than 0.4) and/or a widened AP width (greater than 3 milliseconds) are considered to be significant for ELH. Alteration of the SP and AP in the hydropic ear is believed to result from a mechanical asymmetry in the basilar membrane. Ge and Shea reviewed 1549 patients with MD and found an increased SP/AP ratio in 71.6%. They also showed that the sensitivity of the ECoG increased with duration and severity of disease. The sensitivity increased from 71% in stage 1 disease to 90% in stage 4 disease, and from 43% in MD of less than 1 year duration to 100% when MD had been present for more than 30 years.
The cervical VEMP (cVEMP) is a short latency inhibitory potential of the ipsilateral sternocleidomastoid muscle evoked by a brief and loud (>85 dB) monaural click or tone burst stimuli. The cVEMP is believed to be a recording of the vestibulocollic reflex generated in the saccule, carried via the inferior vestibular nerve. Patients with MD were shown to have increased cVEMP thresholds or absent VEMPs compared with controls. These findings were more common in MD with Tumarkin crisis and were seen in 27% of the contralateral asymptomatic ears of affected individuals. We believe that both VEMP and ECoG should be used to complement the clinical picture and should not be the sole basis for diagnosis.
Caloric Testing and Head-thrust Testing
The role of electronystagmography (ENG) or videonystagmography (VNG) in the diagnosis of MD is limited. Significant caloric weakness is present in 42% to 73% of patients with MD. Complete loss of function is seen in 6% to 11%. Approximately 23% to 29% of patients have abnormal angular vestibulo-ocular reflex (aVOR) on the head-thrust testing (HTT), with gain asymmetry and phase lead being the most common findings.
We believe that caloric testing is useful in: (1) assessment of contralateral function before an ablative procedure, (2) assessment of residual function after an ablative procedure, and (3) assessment of ipsilateral function; if residual function is good, we favor a non-destructive procedure.
Retrocochlear Studies
When surveyed for workup of retrocochlear disorders, 57.7% to 93.3% of otologists obtained retrocochlear studies. We believe that Ménière’s syndrome becomes MD only after excluding other causes; therefore, we obtain MRI on all of our patients.
During the following year, our patient had a total of 5 episodes of severe vertigo associated with aural fullness, hearing loss, and tinnitus. During the course of that year, she developed progression of her hearing loss. The audiogram showed moderate low-frequency hearing loss with a WDS of 72% ( Fig. 7 ). Three of the spells responded to a steroid taper and a regimen of antiemetics. Two episodes were treated with injections of intratympanic dexamethazone (IT Dex) that gave temporary relief of vertigo. Her hearing remained unchanged, and she acquired a hearing aid. Nine months later, she developed recurrence of vertigo spells occurring on a weekly basis. These spells responded less to a combination of oral and intratympanic steroids. A Meniett Device (Medtronic Inc, Minneapolis, MN, USA) was used without success. Her audiogram was unchanged, and she continued to use her hearing aid. At that time, destructive and nondestructive options were discussed as management options for the weekly vertigo spells. She underwent endolymphatic sac decompression with placement of a shunt (endolymphatic sac surgery [ESS]). The sigmoid was noted to be far forward, requiring decompression. The sac was hypoplastic and inferiorly displaced. The surgery resulted in complete resolution of her vertigo spells. Her hearing remained stable. Nevertheless, she continued to complain of moderate to severe roaring tinnitus and constant sensation of aural fullness.
What is the role of medical management?
The medical management of MD includes a low-salt diet, avoidance of caffeine derivatives and alcohol, diuretics, vasodilators, and steroids.
Diuretics and low-sodium diet are effective in controlling the symptoms of MD in 71% to 79% of patients. Although intratympanic gentamicin (IT-Gent) injection is a medical form of therapy, it is a destructive treatment that results in chemical labyrinthectomy.
A Cochrane database review of all prospective randomized controlled trials (RCT), between 1966 and 2005 comparing diuretics with placebo failed to show a single trial of sufficient quality to meet standard criteria set for review. Another Cochrane database review of all RCT comparing betahistine (a vasodilator) with placebo between 1966 and 1999 (6 trials with 162 patients) failed to show any benefit.
Steroids, whether administered orally or topically, have been used to treat acute exacerbations of MD. In a series of 129 patients with unilateral MD, Boleas-Aguirre and colleagues showed that dexamethasone (12 mg/mL) administered intratympanically resulted in vertigo control in 91% of patients. Although more than half of the patients responded to 1 or 2 injections, 21% required more than 4 injections.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


