Chapter 18
IRIS

Injuries of the iris compromise its function as an optical aperture and a mechanical barrier between the AC and the posterior chamber/vitreous. The iris base, along with the ciliary body and angle, is especially sensitive to the shear stress caused by contusion. In open globe injuries, even total aniridia due to actual iris extrusion or subsequent iris retraction may occur.1,2 Discussed separately below are the five major consequences of trauma to the iris:
1. mydriasis;
2. iatrogenic iris laceration;
3. prolapse;
4. iridiodialysis; and
5. aniridia.
| Iatrogenic pharmacological: scopolamine patches3,4 |
| Nightshade5 |
| Aniridia |
| Lack of cholinergic sensitivity |
| Aplasia of the pupillary sphincter and ciliary muscle6,7 |
| Congenital8 |
| Coloboma9 (typical location: inferonasal) |
| Migraine10,11 |
| Siderosis12 (see Chapter 24) |
| Dysgenital disorders (progressive) |
| Iridocorneal endothelial syndrome (iris nevus [Cogan-Reese] syndrome, Chandler’s syndrome, essential progressive iris atrophy13) with pain secondary to corneal edema or secondary angle closure glaucoma |
MYDRIASIS
Pathophysiology
Mydriasis (see Tables 18–1 and 18–2) may be an immediate or late complication of contusion or laceration; it can also occur as a result of head trauma. Mydriasis may present early or late and may be uni- or bilateral. There are various causes of pupil dilatation.
• Sphincter rupture/laceration has been reported from rare sources (water jets, water balloons19,20) and accompanies cataract surgery in 1.321 to 2.3%22 of eyes. It is irreversible, and secondary scarring further restricts pupil motility.
• Third cranial nerve injury may result from uncal herniation causing mechanical compression of the third nerve and subsequent brain stem compromise. A decrease in the brain stem blood flow is another frequent cause.23
• Aberrant cranial nerve regeneration can follow severe head trauma, even if the eye is uninjured. The pupil does not react to light or near but correlates with horizontal gaze. Constriction of the pupil reflects misdirected regeneration of abducens nerve neurons into the parasympathetic pathway of the oculomotor nerve.
• Anterior PVR involves fibrovascular membranes connecting the peripheral retina, ciliary body, and the peripheral iris. Membrane contraction and collagen deposition lead to iris retraction (see Chapter 19 and the Appendix).
| Early | Late | |||
|---|---|---|---|---|
| Anisocoria | Sphincter rupture14 | Anterior PVR15,16 | ||
| Ischemia/compression of the third cranial nerve | Siderosis12 | |||
| Iatrogenic pharmacological mydriasis | Aberrant cranial nerve regeneration17,18 | |||
| Bilateral | Ischemia/compression of the third cranial nerve | |||
| Optic nerve injury19 | ||||
| Iatrogenic pharmacological mydriasis |
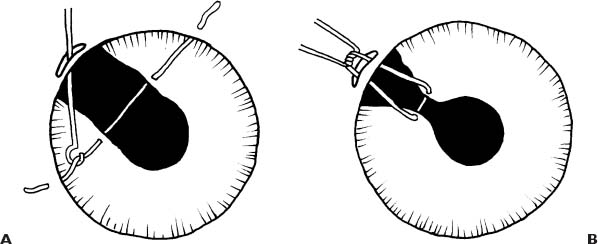
FIGURE 18–1 (A and B) Single iris suture (A). A 9–0 Prolene suture is passed through the limbus and through the iris in line with the proposed suture tract. A bonds hook is introduced through a paracentesis and the two suture ends are drawn out through the wound. (B) A triple throw knot is placed externally and is pulled together with the iris into the corneal wound. The suture ends are cut externally and close to the knot. The sutured iris is pushed back into the AC.
PEARL… It is difficult to free the iris from scar tissue during secondary recon-struction. A thorough primary anterior vitrectomy is much more effective in avoiding iris retraction and anterior PVR in combined anterior/posterior segment injury.
Therapy
If glare and visual deterioration persist, surgical reconstruction should be considered.
• A single suture (Fig. 18–1) constricts the pupil by apposing the sphincter muscle and pupillary margin to each other.24
• A running suture (Fig. 18–2) distributes the forces to the pupillary margin more evenly,25 acting as an “encircling band.” Surgical steps include:
 limbal paracentesis in each quadrant;
limbal paracentesis in each quadrant;
 loosening of posterior synechiae and mobilizing all iris remnants;
loosening of posterior synechiae and mobilizing all iris remnants;
 weaving of a transchamber needle through the iris margin in each quadrant;
weaving of a transchamber needle through the iris margin in each quadrant;
 continuing until the suture is passed through the pupillary margin in all quadrants;
continuing until the suture is passed through the pupillary margin in all quadrants;
 exiting through the first paracentesis and preparing a knot; and
exiting through the first paracentesis and preparing a knot; and
 tightening the knot inside the AC.
tightening the knot inside the AC.
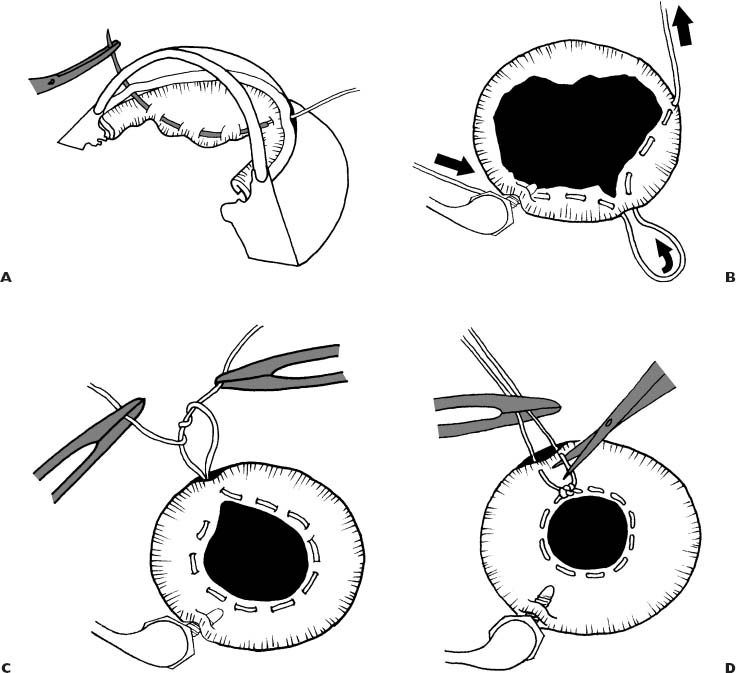
FIGURE 18–2 (A–D) Iris running suture. (A) One limbal paracentesis is placed in each quadrant. The AC is entered with a long, spatula-type, curved transchamber needle, double armed on 10–0 polypropylene. (B) The needle is passed through the iris margin weaving the suture through. After weaving through the iris margin about three to four times, the needle is pulled out through the next paracentesis without damaging the cornea. The needle is then grasped in the same fashion and reentered into the eye through the same incision, and weaving is continued toward the next paracentesis. (C) After exit through the last paracentesis, the knot is tied together, brought into the eye with a hook, and tightened. (D) Following tightening the cerclage suture, the knot is completed and the suture ends cut.
This may occur during phacoemulsification, usually while sculpting anteriorly if the critical distance between the phaco tip and the iris is not maintained. Additional risk factors include atonia/atrophy of the iris, miosis, and high flow. The pigment epithelium or even the stroma may be injured. The consequences include:
• cosmetic problems;
• visual symptoms and peripheral synechia development due to deep sphincterectomy that tend to enlarge with time;
• iridodialysis26; or even
• complete aniridia.a
Therapyb
The need for and type of intervention depend on the lesion. A simple laceration may easily be sutured (McCannel method, see later in this Chapter) using a straight transchamber needle introduced at the limbus through the two iris flaps and out through the limbus on the other side. The needle is cut, and the suture is retrieved through a paracentesis, tightened, and released back into the AC.
PROLAPSE (SEE ALSO CHAPTER 16)
The consequences of prolapse include:
• adhesion to the corneal wound;
• intraocular infection;
• ischemia/necrosis/atrophy;
• goniosynechia and secondary glaucoma (with prolapses at or near the limbus);
• surface epithelization (this starts immediately following the injury,27–29 although epithelial down-growth into the AC, which can be modulated,30 is rare); and
• monocular diplopia (likely to occur when an area of extensive iris resection with an intact pupillary margin is exposed to the palpebral fissure; usually requires suturing).
Therapy
Reposition early to prevent intraocular infection31; in addition to spatula sweeping from the AC, use viscoelastics (see Chapter 16).32 A peripheral iridectomy is advised whenever it is impossible to reposition the iris and to free the angle.
PEARL… Necrosis and surface epithelization are indications for iris resection. This causes less complications than preserving poorly repositioned and nonviable iris tissue. The resulting defect can usually be sutured.24,33
IRIDODIALYSIS
Pathophysiology
Iridodialysis represents a rupture of the iris at its root: the peripheral portion is torn off the ciliary spur. It is typically a consequence of contusion, stretching the iris at and from its insertion. The complaints (glare, monocular double vision) depend on the size of the defect and its position relative to the lid fissure.
Treatment
The most widely used technique is based on the principles of the McCannel34,35
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


