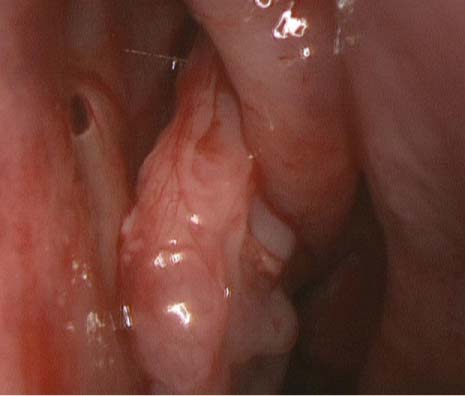
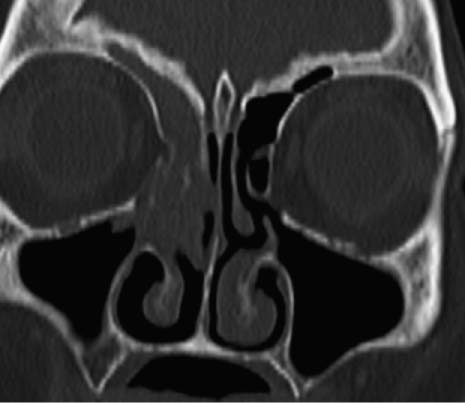
48 A 45-year-old man seen by his primary care physician over several months complains of difficulty breathing through his right nasal cavity for longer than a year, with frequent nasal drainage and occasional bleeding. He is referred after being thoroughly treated for chronic sinusitis with antibiotics and nasal steroid sprays and has had no resolution of his symptoms. He reports having had surgery for a deviated septum and right nasal polyp 2 years ago but has not since been seen by an otolaryngologist. The patient is a social drinker with no smoking history. On examination he appears to have decreased movement of air through his right nasal cavity. Anterior rhinoscopy is essentially clear, but on nasal endoscopy a fairly large polypoid mass can be seen projecting from beneath the right middle turbinate (Fig. 48.1). It appears polypoid and not terribly erythematous, friable, or firm. The mass does not appear to be vascular. Endoscopic examination of the left nasal cavity is clear, demonstrating no evidence of polyps or ostiomeatal disease. A subsequent computed tomography (CT) scan of the sinuses was obtained (Fig. 48.2). 1. The most common nasal mass is a benign inflammatory polyp. However, these tend to be bilateral and have a gray, translucent appearance. The finding of a unilateral nasal mass opens a broad differential that includes infectious processes as well as benign and malignant tumors. Antrochoanal polyps can present as unilateral polypoid masses filling the middle meatus. Benign tumors include osteomas, chondromas, ossifying fibromas, schwannomas, neurofibromas, meningiomas, vascular tumors, hamartomas including ameloblastomas, and, most commonly, papillomas. Malignant tumors of the nasal cavity are most commonly squamous cell cancer but can include adenocarcinoma, esthesioneuroblastoma, lymphoma, melanoma, and others. Fig. 48.1 Right nasal polypoid mass protruding from beneath the middle turbinate. Fig. 48.2 CT demonstrating a polypoid mass within the right anterior ethmoid sinus and middle meatus, with possibly bony disruption of the uncinate process and middle turbinate. 2. Inverting papilloma is a lesion arising from the Schneiderian membrane. This is the transition between the endoderm-derived respiratory epithelium and the ectodermally derived squamous epithelium. Other lesions can arise from this membrane, including fungiform papillomas, which are often found on the nasal septum and are human papillomavirus (HPV) related, and cylindrical papillomas, which appear different but act similar to inverting papillomas. Debate exists as to whether these are different entities or expressions of the same process in different locations. 3. Inverting papillomas histologically have an epithelium that inverts into the underlying connective tissue stroma. They often appear exophytic, polypoid, more vascular than an inflammatory polyp, and with a gray to pink appearance. In contrast to the lesion in this case, they may sometimes appear more fibrous and friable. No mucus cells, koilocytosis, or eosinophils are present. This is in contradistinction to inflammatory nasal polyps. The basement membrane remains intact. Although invasion into surrounding structures such as occurs with malignancy is not present, pressure and mass effect can cause bone remodeling and destruction. 4. Inverting papilloma is the most common benign epithelial tumor of the nose and paranasal sinuses. Incidence is in the range of 0.2 to 0.6% per 100,000 people per year, making up 0.5 to 4% of primary nasal tumors. The male-to-female ratio is 3:1, and predominance in white patients is suggested in the literature. The most common sites of origin include the lateral nasal wall at the root of the middle turbinate and the maxillary sinus. 5.
Inverting Papilloma
History
Differential Diagnosis—Key Points
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


