Intubation
Endotracheal intubation in children with mandibular hypoplasia (Pierre Robin sequence, Treacher Collins syndrome) as well as other craniofacial anomalies has provided a challenge to otolaryngologists and anesthesiologists alike. In addition to the small mandible, several other features of these patients contribute to the difficult intubation: macroglossia, glossoptosis, trismus related to temporomandibular joint abnormalities, and prominent maxillary or mandibular incisors. Most of the traditional techniques that have been described for intubation in problem cases are difficult or impossible to use in infants and young children with mandibular hypoplasia or craniofacial anomalies. We have developed a modification of the standard direct laryngoscopic procedure, utilizing the anterior commissure laryngoscope and an optical stylet in the task of exposing and intubating the larynx of a child with mandibular hypoplasia. This procedure may be used in older children with craniofacial malformations by using appropriately sized instruments.
32-1 Difficult Intubation (Rigid) for the Difficult Airway
Indications
A child with mandibular hypoplasia or other craniofacial anomaly in which standard intubation techniques are unlikely to be successful.
Preoperative Evaluation
Patency of the nasal airway, size of tongue, TMJ mobility, and presence of prominent teeth must be determined preoperatively.
Operative Technique
1. Infants in the first few weeks of life are usually not anesthetized prior to laryngoscopy and intubation. Awake intubation with continuous administration of oxygen is preferred.
2. In older patients, anesthesia is induced using 100% oxygen and an inhalational anesthetic agent or propofol with spontaneous ventilation preserved.
3. Muscle relaxants are best avoided in patients with difficult airway problems.
4. We have chosen to use a 9-cm (pediatric) Holinger anterior commissure laryngoscope for this procedure rather than the various anesthesia laryngoscopes or the Jackson standard laryngoscope. Its straight enclosed barrel design prevents the tongue from obscuring the view of the larynx as so often occurs with the other, more open instruments. In addition, its narrow profile throughout its entire length permits easier access to the laryngeal inlet and allows the barrel of the laryngoscope to slip more completely laterally into the oral commissure. Suctioning of excess secretions can be performed easily through this instrument using a straight laryngoscopic suction. Other techniques that utilize curved laryngoscopic blades, blind intubation, or flexible fiberoptic laryngoscopes do not allow such complete and easy clearing of pharyngeal secretions.
5. The dicta of Jackson regarding the position of the patient are still of prime importance. The patient is supine with the head elevated above the shoulders. The neck is flexed forward and the head extended at the atlanto-occipital joint to bring the axes of the mouth, pharynx, and larynx into alignment.
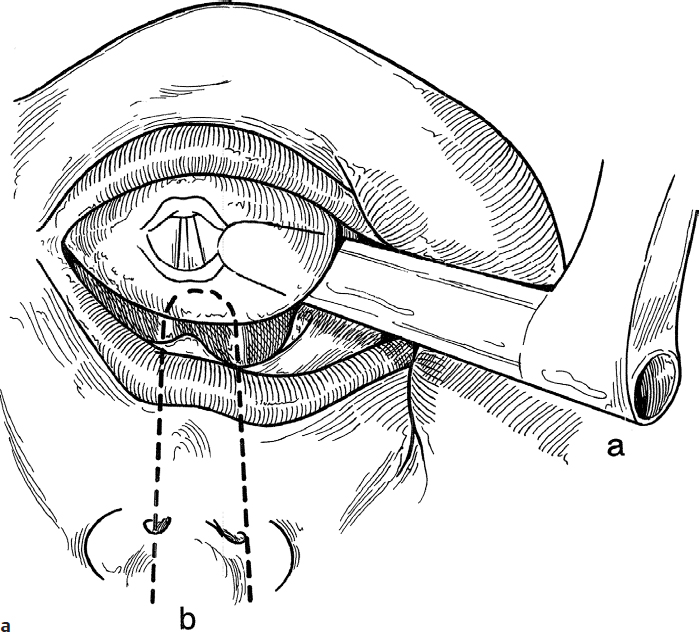
6. The laryngoscope is introduced into the mouth and advanced along the right side of the anterior two-thirds of the tongue (Fig. 32.1a, position a).
7. Instead of shifting the whole laryngoscope toward the mid-line in the traditional manner (Fig. 32.1a, position b), only the laryngoscope tip is directed toward the midline, while the proximal end is shifted far laterally into the oral commissure. This allows 20–30 degrees of additional anterior angulation of the blade (Fig. 32.1b, position a). This anterior angulation is not possible with the laryngoscope in the standard midline position because of the bulky tongue, hypoplastic mandible, and the prominent maxilla or maxillary teeth common in these children (Fig. 32.1b, position b).
8. With the instrument approaching the larynx from the right side, the epiglottis is visualized and elevated with the tip of the laryngoscope.
9. Visualization of the larynx within the lumen of the laryngoscope may be facilitated by external pressure over the cricoid area in the posterior and lateral (toward the laryngoscope) direction.
10. With the larynx visualized, placement of an endotracheal tube requires a special sequence of maneuvers.
a. The 15-mm adapter is removed from a tube of appropriate size and a water-soluble lubricant is placed on the outside of the tube to facilitate movement of the tube within the barrel of the laryngoscope.
b. The tube is placed in the lumen of the laryngoscope and passed beyond the vocal cords.
c. This step may be aided by the use of an optical stylet (2.7-mm diameter telescope, 27018A Karl Storz Endoscopy-America, Inc.) placed inside the endotracheal tube (Fig. 32.1c). (If a stylet is used, it should also be coated with a water-soluble lubricant to promote easy insertion into and removal from the endotracheal tube.)
d. The proximal end of the endotracheal tube is grasped and stabilized in its position with a laryngeal alligator forceps as the laryngoscope is withdrawn (Fig. 32.1d).
e. The 15-mm adapter is reinserted into the endotracheal tube and ventilation is commenced in the usual manner (Fig. 32.1e).
f. Placement of the endotracheal tube in the trachea is confirmed by auscultation for bilateral air entry and observation of bilateral chest movement.
Complications
1. Laryngospasm
2. Glottic edema
3. Dental trauma