and Mitrofanis Pavlidis2
(1)
Department of Ophthalmology, Uppsala University Hospital, Uppsala, Sweden
(2)
Augencentrum Köln, Cologne, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-20236-5_1) contains supplementary material, which is available to authorized users.
Electronic supplementary material
for this chapter is accessible online at http://extras.springer.com/ by searching via the ISBN.
Trocar Against No Trocar
The most essential development of small-gauge vitrectomy was the introduction of a trocar which rests inside the sclera. Instruments are much easier introduced, the trocar protects the sclera against injury through the instruments and a trocar is easier to find than a usual sclerotomy. The disadvantage of the trocar compared to the usual sclerotomy is the excessive leakage of fluid through the trocars.
Valve Against No Valve
The valve on the trocar solves this problem. The valve keeps the globe watertight. You can remove the infusion and the globe is still normotensive. Valves have more advantages. Valves prevent incarceration of vitreous into the trocars; less fluid is infused; valves build up a higher intraocular pressure, which is useful during a fluid–air exchange or removal of a preretinal oil bubble; and you do not need to work with plugs.
1.1 Does Size Matter?
We are convinced that size does matter. See Table 1.1. Size was the major motivator to switch from ECCE to phacoemulsification. The small incisions of phacoemulsification are better in almost all aspects than the gaping wound of ECCE: faster postoperative recovery, improved visual results, less astigmatism and a closed and safe globe.
Table 1.1
Outer diameter of a needle in gauge and mm
Gauge | External diameter in mm |
|---|---|
17 | 1.4 |
19 | 1.07 |
20 | 0.9 |
23 | 0.64 |
25 | 0.51 |
27 | 0.41 |
29 | 0.34 |
30 | 0.30 |
The same principle applies for vitrectomy. Small sclerotomies and small instruments induce less intraoperative trauma, improved postoperative gas filling, less leakage and faster postoperative recovery. The principle “the smaller the gauge, the better” is evident.
The main disadvantage of 23G is that the sclerotomies are not as tight as 20G sclerotomies with sutures. The use of 23G is thought to be a sutureless technique but requires quite often sutures in order to avoid postoperative hypotony.
Don’t Forget
A 27G trocar creates a 25G sclerotomy. A 25G trocar has a 23G sclerotomy. And a 23G trocar has a 22G sclerotomy. It is obvious, that a 25G sclerotomy is superior to a 22G sclerotomy.
27G, in contrast, has no leakage, the globe is watertight without sutures, and the tiny instruments cause less intraoperative trauma (Figs. 1.1, 1.2, 1.3, and 1.4). The major advantages are as follows:
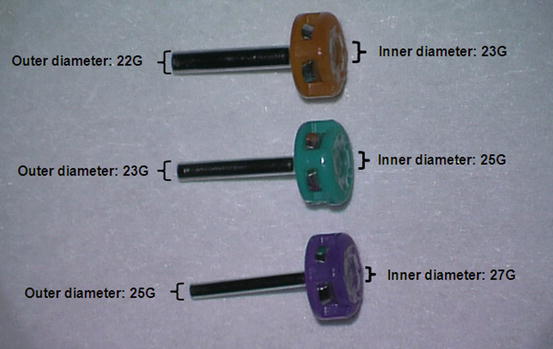
Fig. 1.1
The inner diameter of a 23G trocar is 23G but the outer diameter is 22G. A 23G trocar has therefore a 22G sclerotomy. The outer diameter of a 27G trocar is 25G. It is obvious that a 25G sclerotomy is water-tighter than a 22G sclerotomy