Purpose
To assess the effects of intravitreal ranibizumab injection in patients affected by pigment epithelial detachment associated with occult subfoveal choroidal neovascularization.
Design
Prospective, interventional case series.
Methods
Participants: Forty eyes of 40 patients were considered for the purpose of the study. Consecutive patients were recruited for a 24-month study. All patients underwent a complete ophthalmic examination, including best-corrected visual acuity on Early Treatment Diabetic Retinopathy Study (ETDRS) charts. After a 3-monthly loading phase, further intravitreal ranibizumab injections were administered on the basis of detection of any type of fluid on optical coherence tomography. Primary outcome measures: Changes in mean best-corrected visual acuity at 12 and 24 months and the proportion of eyes losing fewer than 15 letters (corresponding to 3 ETDRS lines) from baseline visual acuity. Secondary outcome measures: Changes in central macular thickness on optical coherence tomography and variation in mean area of the entire lesion.
Results
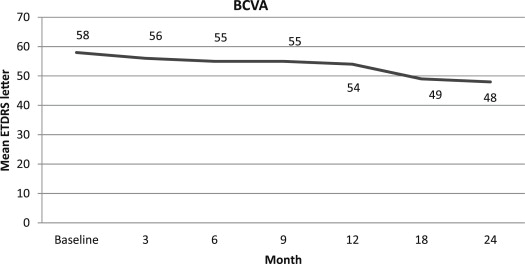
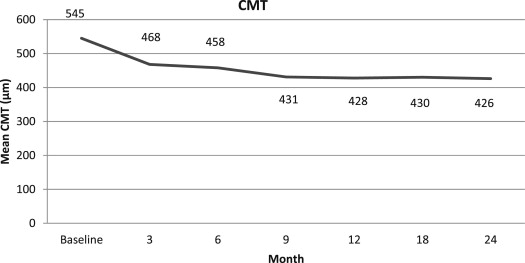
Forty patients were included. Mean best-corrected visual acuity decreased from 20/66 (58 ETDRS letters) to 20/83 (53 letters) at 12 months and 20/112 (489 ETDRS letters) at 24 months ( P = .003). Eighty percent and 67.5% of eyes lost fewer than 3 lines at 12 and 24 months, respectively. Mean central macular thickness passed from 545 μm to 428 μm at 12 months and 426 μm at 24 months. Mean lesion area changed from 6826 μm 2 to 6312 μm 2 at 12 months and 6010 μm 2 at 24 months.
Conclusions
The treatment of pigment epithelial detachment associated with occult subfoveal choroidal neovascularization with intravitreal ranibizumab injection after a 3-monthly loading phase and pro re nata strategy can lead to partial results over a 24-month follow-up. Further investigations are warranted to establish the best therapeutic approach to this disease.
Pigment epithelial detachment (PED) may complicate age-related macular degeneration (AMD), especially when associated with choroidal neovascularization (CNV). The management of vascularized PED is still controversial. Whereas the natural history is generally poor, the various treatments proposed, including laser photocoagulation, photodynamic therapy, intravitreal triamcinolone acetonide, and combined therapy, have provided limited benefits. A more recent approach is based on the intravitreal administration of anti-vascular endothelial growth factor (VEGF) inhibitors. The aim of the present study is to assess the effects of intravitreal ranibizumab injection in patients affected by PED associated with occult subfoveal CNV.
Methods
The study was designed as a prospective, nonrandomized, open-label, interventional case series with a scheduled follow-up of 24 months. Patients affected by PED associated with occult subfoveal CNV secondary to AMD were enrolled prospectively from January 2008. The inclusion criteria used for the recruitment of patients were: diagnosis of vascularized PED in AMD, best-corrected visual acuity (BCVA) between 1.30 to 0.30 logarithm of the minimal angle of resolution units (corresponding to approximately 20/400 to 20/40 Snellen), identification of occult subfoveal CNV on indocyanine green angiography (ICGA), and willingness to sign written informed consent. Exclusion criteria comprised any previous treatment (i.e., laser, photodynamic therapy, intravitreal triamcinolone acetonide, anti-VEGF injection), presence of any other ocular disorder able to confound the clinical assessment, identification of a retinal angiomatous proliferation on ICGA, and media opacities.
The patients underwent a complete ophthalmic examination, including determination of BCVA on standard Early Treatment Diabetic Retinopathy Study (ETDRS) logarithm of the minimal angle of resolution charts, anterior segment slit-lamp examination, dilated fundus biomicroscopy, spectral-domain optical coherence tomography (OCT), fluorescein angiography, and ICGA. OCT (Spectral OCT SLO; Opko/OTI Inc, Miami, Florida, USA) was performed using a scan line pattern. Central macular thickness (CMT) was calculated manually, measuring the distance between the Bruch membrane and the internal limiting membrane, centering the examination on the fovea. Fluorescein angiography and ICGA were performed using a scanning laser ophthalmoscopy (Heidelberg Retina Angiograph; Heidelberg Engineering, Heidelberg, Germany). The total lesion area (including PED, blood, and exudation) was outlined manually with the computer mouse using the option provided by the software, and the results were expressed in square micrometers. BCVA assessment, fundus biomicroscopy, and OCT scans were performed by ophthalmologists masked to the patient’s condition (LP, MC, and MG). Analyses of angiographic frames and OCT scans were conducted independently by 2 trained ophthalmologists masked to the patient’s clinical characteristics (AP and SDK). Uncertain cases were reviewed by a third ophthalmologist (FB).
The treatment regimen provided a loading phase of 3-monthly intravitreal ranibizumab injections, followed by further injections on the basis of detection of any type of fluid on OCT revealing the presence of subretinal fluid (SRF), intraretinal fluid (IRF), and persistence or recurrence of PED. All patients were re-evaluated monthly up to the end of the 24-month follow-up. According to the protocol, OCT examination was performed monthly, fluorescein angiography and ICGA were performed quarterly, and additional angiographies were possible at the examiner’s discretion. The primary outcome measures were the changes in mean BCVA at 12 and 24 months and the proportion of eyes losing fewer than 15 letters (corresponding to 3 ETDRS lines) from baseline visual acuity. Secondary outcomes included the changes in both the mean CMT on OCT and in the mean total lesion area.
Statistical analysis was performed using the Student t test (paired and unpaired depending on the groups) to evaluate the changes in BCVA, CMT, and total lesion area and using the chi-square test for the comparison of proportion. Regression analysis was applied to assess the relationship between BCVA and morphologic parameters. All tests were 2-tailed, and the level of significance was taken at P < .05.
Results
Forty-nine patients were considered for the study, but only 40 patients (23 females) were enrolled because 9 patients displayed PED associated with retinal angiomatous proliferation on ICGA. Mean age was 78 ± 8 years. In all cases, the PED was localized in the foveal area. The adherence of the patients to the scheduled visit examination through the 24-month follow-up was quite good. Indeed, at the end of the follow-up, only 20 patients missed 2 visits, whereas 17 missed a single visit. No patient missed 2 consecutive visits.
Mean BCVA ± SD at baseline was 58 ± 14 ETDRS letters (corresponding to approximately 20/66 Snellen) and worsened to 53 ± 17 ETDRS letters at 12 months (corresponding to approximately 20/83 Snellen; P = .013) and to 48 ± 16 letters at 24 months (corresponding approximately to 20/112 Snellen), with a statistically significant difference with respect to baseline ( P = .0001; Figure 1 ). Thirty-two (80%) and 27 (67.5%) eyes lost fewer than 3 ETDRS lines from baseline visual acuity at 12 and 24 months, respectively ( Table 1 ). Eight patients (20%) and 13 patients (32.5%) showed a 3-line loss at 12 and 24 months, respectively. A single patient (2.5%) obtained a 3-line BCVA improvement both at 12 and 24 months. Mean line loss was 1.02 ± 2.31 and 2.28 ± 3 at 12 and 24 months, respectively. Mean CMT was 545 ± 228 μm at baseline, changing to 428 ± 168 μm at 12 months ( P = .001) and 426 ± 177 μm at 24 months ( P = .001; Figure 2 ). Mean total lesion area was 6826 ± 3664 μm 2 at baseline, changing to 6312 ± 3296 μm 2 at 12 months ( P = .08) and to 6010 ± 3078 μm 2 at 24 months, reaching a statistically significant difference at the end of the follow-up ( P = .01).
| Change in Visual Acuity | 12 Months | 24 Months |
|---|---|---|
| ≥ 3-line increase | 1 (2.5%) | 1 (2.5%) |
| ≥ 1-line to < 3-line increase | 8 (20%) | 5 (12.5%) |
| No variation | 9 (22.5%) | 6 (15%) |
| ≥ 1-line to < 3-line decrease | 14 (35%) | 15 (37.5%) |
| ≥ 3-line decrease | 8 (20%) | 13 (32.5%) |
Regression analysis revealed a statistically significant correlation between BCVA and CMT at baseline ( P = .037) and at the 24-month visit ( P = .005). At the same time points, no statistically significant correlation linked BCVA and total lesion area ( P = .33 at baseline and P = .48 at 24 months).
The mean number of intravitreal ranibizumab injections was 7.1 through 12 months (range, 3 to 11) and 14.9 through 24 months (range, 3 to 23).
At the end of the follow-up, PED persistence and PED resolution were observed in 31 eyes (77.5%) and 9 eyes (22.5%), respectively ( Table 2 ). Subgroup analysis disclosed no statistically significant difference regarding baseline BCVA, CMT, and lesion area, comparing the 2 subgroups characterized by either PED persistence or PED resolution. Over the course of the follow-up, BCVA showed a statistically significant worsening in both subgroups, although the subgroup with PED resolution exhibited a lower reduction than eyes with PED persistence. A statistically significant reduction in CMT was achieved in both subgroups. Although CMT did not differ between the subgroups at the baseline, a larger improvement in CMT was noted at the 24-month examination in favor of the subgroup showing PED resolution. The mean total lesion area reduced from 6603 ± 3157 μm 2 to 6074 ± 2954 μm 2 and from 7591 ± 5213 μm 2 to 5787 ± 3657 μm 2 in the subgroups with PED persistence and PED resolution, respectively. There was no statistically significant difference between the subgroups over the course of the follow-up and at the final visit. A mean of 7.7 injections were administered in the subgroup with PED persistence through the first year, and a mean of 16.8 injections were administered in the subgroup with PED persistence through the second year. A statistically significant lower number of injections (5.1 and 8.4, respectively) were administered in the same period in eyes with PED resolution.
| PED Persistence | PED Resolution | P Value | |
|---|---|---|---|
| No. of eyes (%) | 31 (77.5) | 9 (22.5) | |
| BCVA (mean ± SD, logMAR) | |||
| Baseline | 0.53 ± 0.28 | 0.51 ± 0.25 | .79 |
| 24 mos | 0.77 ± 0.34 (0.001) a | 0.64 ± 0.21 (0.04) a | .28 |
| Loss ≥ 3 lines | 12 (38%) | 1 (11%) | .22 |
| CMT (mean ± SD, μm) | |||
| Baseline | 574 ± 238 | 443 ± 160 | .13 |
| 24 mos | 476 ± 169 (0.01) a | 251 ± 22 (0.01) a | .001 |
| Area (mean ± SD, μm 2 ) | |||
| Baseline | 6603 ± 3157 | 7591 ± 5213 | .57 |
| 24 mos | 6074 ± 2954 (0.09) a | 5787 ± 3657 (0.06) a | .79 |
| No. of injections (mean) | |||
| 12 mos | 7.7 | 5.1 | .01 |
| 24 mos | 16.8 | 8.4 | <.001 |
a P value regarding the comparison with the corresponding baseline values.
Additional subgroup analyses were performed in accordance with the final BCVA variations. Two subgroups were established: one showing a stable or improved BCVA at the last visit (no variation or gain of 1 letter), an the other showing a decline in BCVA (final loss of at least 1 letter). Nine (22.5%) patients were included in the improved BCVA subgroup and 31 (77.5%) patients were included in the stable BCVA subgroup. Median and mean BCVA differed significantly at the baseline, with the lower BCVA values in the improved BCVA subgroup ( P = .03; complete data are listed in Table 3 ). Although no statistically significant difference could be demonstrated, at the baseline and final examination, both the CMT and total lesion area readings were higher in the improved BCVA subgroup than in the stable BCVA subgroup. The clinical history evidenced a significant difference between the 2 subgroups with regard to symptom duration before the diagnosis, the longer duration occurring in the subgroup showing a final BCVA loss (11 ± 5 days vs 21 ± 11 days; P = .02). During the follow-up, 2 patients (0.5%) demonstrated a retinal pigment epithelium tear at the third intravitreal ranibizumab injection. No other ocular or systemic side effects were registered over the follow-up.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


