Intrastromal Implants for Keratoconus
Joseph Colin
Keratoconus is a noninflammatory, progressive, ectatic, and thinning disease of the cornea that has been studied extensively, but the underlying mechanisms of stromal thinning are not well understood. Recent work suggests that the loss of corneal stromal tissue may be caused by increased levels and activity of proteases or decreased levels of inhibitors of protease activity. Epithelial injury resulting from trauma or refractive surgery may also cause loss of anterior stromal keratocytes through apoptosis modulated by interleukin-1 (1,2).
Noninvasive treatment modalities such as spectacles and contact lenses can provide functional vision in the early stages of this progressive disease (3, 4, 5). These modalities are less effective in correcting severe corneal irregular astigmatism and stromal opacities. Penetrating keratoplasty (PK) may be needed to restore visual function, particularly in the presence of marked central opacities (6, 7, 8, 9). Patients suffering from irregular astigmatism without corneal opacities may be reluctant to pursue PK, and may seek less invasive interventions to improve best corrected spectacle visual acuity (BCVA) or uncorrected visual acuity (UCVA). These include lamellar keratoplasty, epikeratoplasty, phakic intraocular lenses (IOLs), and intrastromal corneal rings.
Incisional and excimer laser refractive surgery keratorefractive procedures are contraindicated in keratoconus. Incisional surgery (radial keratotomy and astigmatic keratotomy) and ablative corneal procedures [photorefractive keratectomy (PRK) and laser-assisted in situ keratomileusis (LASIK)] may induce intraoperative complications and may have an unacceptably high rate of unpredictability and instability (10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23).
TREATMENT OPTIONS
PK provides good visual outcomes for most patients with keratoconus. However, visual rehabilitation is slow, there is constant endothelial cell loss, and keratoconus may recur 15 to 20 years later. In patients with Down’s syndrome, known to have a high frequency of keratoconus, the risk of serious complications after PK is considerably increased because of poor cooperation and extensive eye rubbing.
Deep lamellar keratoplasty can be used to decrease the incidence of graft rejection after PK (24). Air is injected into the corneal stroma, expanding its normal thickness as much as threefold. Lamellar dissection is performed as deeply as possible, close to Descemet’s membrane. The rehydrated donor button is sutured in place with interrupted monofilament sutures. The surgical technique is more demanding than PK. The advantages compared with PK include preservation of the endothelium, no graft rejection, more rapid wound healing, and short duration of topical corticosteroid regimen.
Plano epikeratoplasty adds healthy donor tissue, thereby flattening the ectatic cornea and supporting the bulged corneal dome (14,17, 18, 19,25,26). Krumeich et al. used epikeratoplasty for the treatment of mild and moderate keratoconus, and reported that progression of the disease was arrested in some cases (26). If epikeratoplasty is unsuccessful, the patient may safely undergo PK at a later date.
Wagoner et al. compared the results of 443 eyes that received PK with 161 eyes treated with epikeratoplasty (19). With at least 2 years of postoperative follow-up data, the study showed PK provided better visual outcomes, but the results with epikeratoplasty were sufficiently good to recommend its use as a surgical alternative in cases when PK was not desirable (certain lifestyle demands and Down’s syndrome).
A retrospective study compared the results of epikeratophakia with PK and LP for patients with keratoconus. Epikeratophakia was recommended as the grafting procedure of choice in most patients; however, in selected cases, PK may be performed with better functional results, if uncomplicated (4).
Phakic refractive IOLs are easily implanted and provide predictable refractive and visual results in myopic patients. The implantation of a refractive IOL is a refractive surgical option in patients with early keratoconus, high myopia, and minimal astigmatism. The surgery is facilitated by the greater anterior chamber in keratoconus.
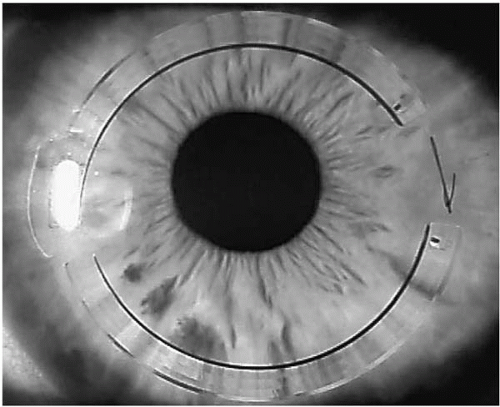 FIGURE 64-1. Slit-lamp aspect of the keratoconic cornea after Intacs implantation.(see color image) |
Intrastromal corneal rings were initially used for the correction of low myopia (22,27, 28, 29, 30). They act as passive spacing elements that shorten the arc length of the anterior corneal surface, flattening the central cornea (23,31). This biomechanical effect is expected to be greater in keratoconic eyes, which have thinner corneas.
Now supplied by Addition Technology of Fremont, California, Intacs prescription inserts are delivered in boxes containing two segments of the same thickness. In Europe, Intacs intrastromal corneal rings are available in 11 sizes, ranging from 0.21 to 0.45 mm. In the United States, the rings are available in five sizes, from 0.25 mm to 0.35 mm.
The major objective is to reshape keratoconic corneas with two Intacs inserts of differing thickness. Intacs inserts are applied to lift the inferior ectasia and flatten the soft keratoconic corneal tissue in an attempt to decrease the asymmetric astigmatism induced by keratoconus, without removing any corneal tissue or touching the central cornea (Fig. 64-1). The rings may be explanted if needed.
Intacs inserts do not eliminate the corneal disease but they may improve visual acuity, and delay or eliminate the need for corneal transplantation. The best candidates are keratoconic patients with contact lens intolerance and a clear central cornea. In patients with apical and superficial opacities, phototherapeutic ablation may be performed before Intacs implantation.
EARLY INTACS STUDIES
Research indicates that Intacs implantation is safe and effective for keratoconic eyes. Most patients experience improved BCVA and UCVA, with a very low risk of complications. Colin et al. performed the first Intacs implantation into keratoconic eyes in June 1997 (20). The surgery was performed in patients with clear central corneas and contact lens intolerance. The spherical equivalent error and refractive astigmatism were significantly reduced after surgery, topographic regularity was increased, and UCVA was improved in almost all patients, at all postoperative time points examined (p ≤ .05). BCVA and UCVA values are presented in Table 64-1. Topographic corneal shape (size and height of the cone) was improved for all subjects compared with baseline measurements. Average postoperative mean keratometry was reduced by approximately 3 diopters (D), and mean keratometric astigmatism decreased steadily over postoperative time points (Figs. 64-2 and 64-3).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


