Purpose
To describe the use of high-resolution anterior segment optical coherence tomography (AS-OCT) during deep anterior lamellar keratoplasty (DALK).
Design
Prospective case series.
Methods
At the Singapore National Eye Centre we performed sequential intraoperative AS-OCT scans using iVue 100-2 (Optovue, Fremont, CA, USA) during various DALK techniques.
Results
In case 1 (corneal scarring) the OCT images helped to guide manual dissection, showed the depth of the needle track before air injection, and identified the location of a small bubble when the big bubble failed. In cases 2 (macular dystrophy) and 3 (lattice), viscodissection was undertaken, but in case 2 the OCT showed the viscoelastic trapped intrastromally, compared to case 3, in which the viscobubble dissection was successful. In case 4 (irregular corneal thinning and scarring), AS-OCT enabled accurate decision on initial trephination and guided dissection. In case 5 (keratoconus), the OCT showed the achieved big-bubble and detached Descemet membrane. Case 6 was a repeat DALK; the OCT guided the manual dissection of the residual stroma underlying the failed graft. In case 7, the OCT showed an intrastromal retention of fluid that was not detectable by the operating microscope due to diffuse scarring following alkaline injury. The OCT helped to assess the location of the Descemet membrane and guided the manual dissection.
Conclusions
Intraoperative high-definition AS-OCT obtained good-quality images of the cornea during DALK and proved useful in various cases of DALK to help the surgeon decide on a number of surgical steps.
Recent improvements in surgical techniques and technology have led to the resurgence of deep anterior lamellar keratoplasty (DALK) as an alternative to penetrating keratoplasty (PK) for the treatment of corneal stromal diseases for a variety of optical, tectonic and therapeutic indications. A recent review has established that DALK is superior to PK in preserving corneal endothelium and is therefore the preferred option for patients experiencing corneal stromal disease that does not affect the endothelium. Even while taking into consideration the differing complications and outcomes of DALK and PK, DALK has been shown to be a more cost-effective procedure.
Visual acuity results of DALK have been shown to be better if a bare Descemet membrane is achieved or if there is minimal residual stroma, as in a predescemetic DALK. Variations of the big-bubble technique first introduced by Anwar have been described. In our centre, we use a modified technique in which an anterior stromal layer is removed before attempting the big-bubble. The depth of the initial trephination is routinely decided based on the ultrasound pachymetry, aiming to leave a residual stroma of approximately 150 μm to allow for the safe placement of the 27-gauge needle closer to the Descemet membrane. In our technique, a needle is first used to create the initial tunnel in the stroma advancing for 2–3mm. A blunt cannula (Tan DALK cannula 27 gauge, AE-7803; Asico, Westmont, IL, USA) attached to a 3 or 5 mL air-filled syringe is then introduced through that initial opening. It is advanced 1 mm farther toward the Descemet membrane before injection of air is commenced.
The initial manual dissection and the use of a blunt cannula allows for a safer air-injection with reduced risk for perforation. However, in cases of marked irregular thinning, the ultrasound pachymetry can provide only an estimate of the corneal thickness and the location of the thinning, which can lead to an inadequate depth of trephination and manual dissection, increasing the risk for obtaining too thin a residual stroma for the safe introduction of the needle/cannula, or even an undesired perforation. Also, in cases where the injection of air does not achieve the desired Descemet membrane separation, the surgeon is left with an emphysematous whitened cornea, in which visualization is impaired and ultrasound pachymetry may not obtain reliable measurements. The surgeon may then try a viscodissection or continue with another layer of manual dissection without knowing the real depth and evenness of the dissection. This increases the risk for perforation and for irregular residual stroma that may affect the final postoperative visual acuity.
Anterior segment optical coherence tomography (AS-OCT) allows for rapid, noncontact, high-resolution imaging of the anterior segment. Intraoperative AS-OCT imaging has been shown to be useful during Descemet stripping automated endothelial keratoplasty (DSAEK) to detect the presence of interface fluid and assess the effect of the procedure and air tamponade on graft thickness. In this study, we assessed the utility of intraoperative AS-OCT during DALK surgery: whether it could help reduce the risk for perforation and for uneven residual stroma and guide the surgeon intraoperatively in various surgical steps in cases where the surgery is more complicated.
Methods
We conducted a prospective study of patients undergoing DALK for a variety of corneal diseases at the Singapore National Eye Center between November 2011 and March 2012. Informed consent was obtained from all subjects to participate in this prospective study, which followed the principles of the Declaration of Helsinki, and ethics approval was obtained from the Singapore Health Services Institutional Review Board in accordance with their guidelines.
Depending on the condition of each eye, either a modified big-bubble technique, as described in the introduction, or a manual dissection was planned. Surgeries were performed by 2 experienced corneal surgeons (J.S.M. and D.TH.T). Intraoperative AS-OCT imaging was performed during several steps of the surgery, using the spectral domain OCT (iVue 100-2; Optovue, Fremont, CA, USA) in the dark operating theater. All scans were performed by 1 independent observer (LBL), who optimized each scan for the best image quality. We used the standard anterior segment single-scan protocol with multiple horizontal scans, ie, 26,000 axial scans per second, scanning width of 6 mm and 5 μm image resolution. We have previously described the use of this device in DSAEK surgery; however, this device is now supported by a microscope arm, and a pedal allows it to be aligned in the X, Y, and Z axes.
Results
Included in the study were 7 eyes of 7 Asian patients; their mean age was 31.5 ± 16.5 years.
Case 1, Manual Dissection
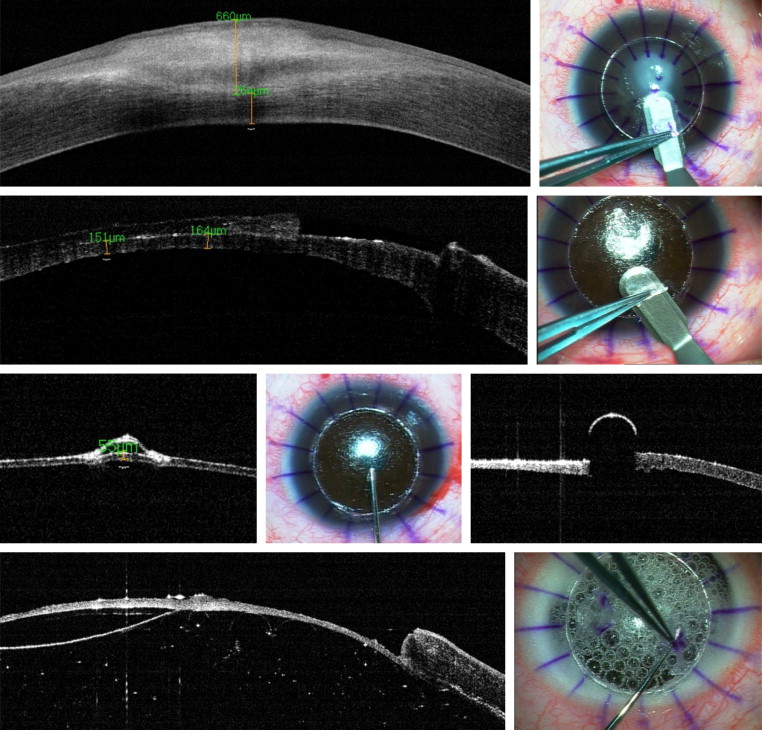
A 9-year-old male with corneal scarring secondary to neurotrophic keratopathy underwent DALK ( Fig. 1 , top left). The described modified big-bubble technique was used, starting with partial trephination and dissection ( Fig. 1 , top right). In this case, the residual thickness shown by the OCT was 250 μm, so a further manual dissection was undertaken, leaving a posterior residual stroma of approximately 150 μm ( Fig. 1 , second line). A 27-gauge needle was used to create the initial opening, and the depth of the track was assessed with the AS-OCT imaging ( Fig. 1 , third line, left). A blunt cannula was introduced through that initial opening in the stroma, attached to an air-filled syringe ( Fig. 1 , third line, center); the OCT image, however, could not show the underlying structures beneath the metallic cannula ( Fig. 1 , third line, right). After air injection, the surgeon suspected that only a small, localized air bubble had been attained, but visualization under the operating microscope could not confirm it. The OCT confirmed its presence and location ( Fig. 1 , bottom left). However, in view of his young age, the surgeon decided to avoid any risk for perforation and did not dissect the small bubble, undertaking instead an OCT-guided predescemetic manual dissection ( Fig. 1 , bottom right). The surgery was successfully completed, leaving 50 μm of residual stroma and leaving the area of the bubble to reabsorb.
Case 2, Failed Viscodissection
A 57-year-old male with lattice dystrophy underwent DALK with initial succesful trephination and dissection, but a big bubble was not achieved. A dispersive ophthalmic viscosurgical device (Viscoat; Alcon Laboratories, Hünenberg, Switzerland) was used to perform a viscodissection. With this, a bubble was achieved, but due to the difficult visualization under the surgical microscope through the viscohydrated cornea, the surgeon could not identify whether it was intrastromal or whether dissection at the Descemet plane had been achieved. The OCT image at this stage showed that the viscoelastic had created an intrastromal separation of the corneal lamellae, with no Descemet membrane separation ( Supplemental Fig. 1 ). Further manual dissection was therefore undertaken, with the help of the intraoperative OCT to guide the depth of dissection. Finally, the Descemet plane was reached, and a descemetic dissection successfully achieved.
Case 3, Successful Viscodissection
In this case of macular dystrophy in a 38-year-old male, a DALK was scheduled because endothelial function was still preserved. However, a big bubble was not achieved, and multiple small air bubbles could be detected separating the stroma from the Descemet membrane on AS-OCT ( Supplemental Fig. 2 ). The surgeon decided to attempt viscodissection, which proved successful and, although the OCT could not show the viscobubble, it did not show any intrastromal accumulation of the viscoelastic, and the surgeon could complete the baring of the Descemet membrane without complications.
Case 4, Irregular Corneal Thinning
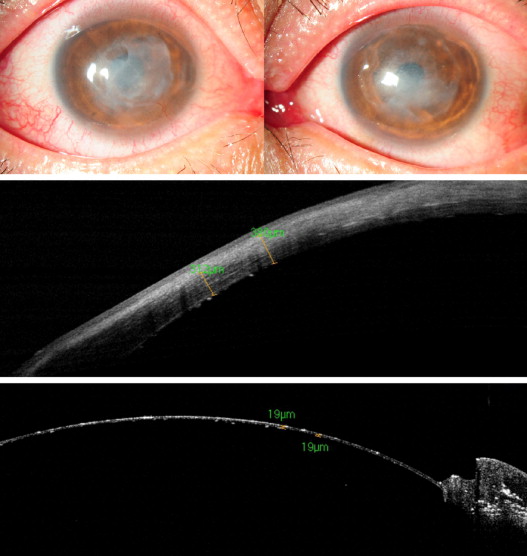
A 41-year-old male suffered bilateral corneal scarring and irregular thinning after corneal infections following epipolis laser in situ keratomileusis (epi-LASIK) surgery ( Fig. 2 , top). Intraoperative AS-OCT revealed 312 μm of stroma in the thinnest point (under the epithelium) in contrast to ultrasound pachymetry of 450 μm (with epithelium) ( Fig. 2 , middle). Based on this, the surgeon decided to trephine initially only up to 200 microns, to avoid perforation. Manual dissection was then undertaken, guided by repeated OCT images, until it showed a residual stroma of 200 to 300 μm in different parts of the cornea. A big bubble was then attempted and achieved, and the residual stroma was removed, leaving a bare Descemet membrane ( Fig. 2 , bottom).
Case 5, Big Bubble
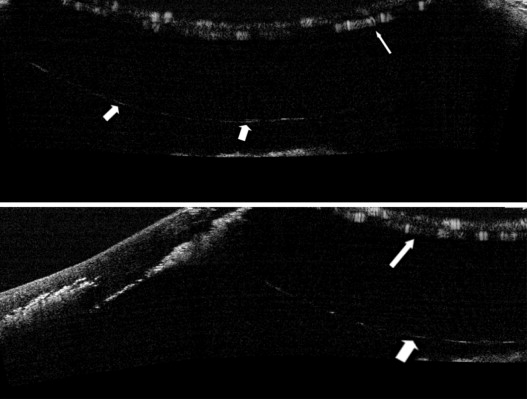
In this 30-year-old male with keratoconus and no previous history of hydrops, the big bubble was achieved and imaged with the AS-OCT ( Fig. 3 ). The air bubble could be seen close to the iris and the anterior capsule of the lens, but because the scan had to be focused much deeper to detect the bubble, and the depth of the image obtained with the OCT was limited, we could not get a single image that included both the cornea and the big bubble together. Surgeons desiring to detect the bubble with the OCT need to be aware that the scan has to be focused significantly posteriorly to detect the bubble and Descemet membrane separation.
Case 6, Manual Dissection
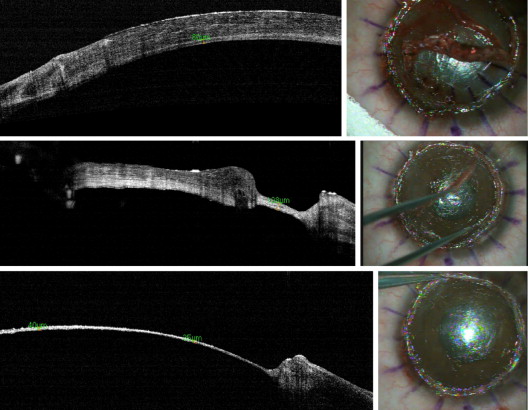
In this 22-year-old female with a previous failed DALK, intraoperative AS-OCT revealed 80 μm of posterior lamella underneath the failed DALK ( Fig. 4 , top left). Careful manual dissection was performed ( Fig. 4 , top right) until the interface separating the failed graft and the recipient’s cornea was reached ( Fig. 4 , middle), and the graft was safely removed. The residual layer of the recipient’s cornea had become vascularized following rejection of the graft. Further manual dissection was then undertaken, guided by OCT, to remove the vascularized stroma, leaving a clear residual stromal thickness of 40 μm ( Fig. 4 , bottom).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


