Purpose
To compare the intraocular pressure (IOP) values during a 3-month period after implantation of the new Visian Implantable Collamer Lens (ICL; STAAR Surgical Company, Nidau, Switzerland) V4c design with CentraFLOW technology without iridotomy using a standard procedure followed by implantation of the conventional ICL V4b model.
Design
Retrospective cohort study.
Methods
This study included 17 eyes implanted with the ICL V4b model and 18 eyes implanted with the ICL V4c model. The mean preoperative spherical equivalent refractions were −7.48 ± 5.00 diopters and −8.66 ± 4.2 diopters, respectively. We compared the best-corrected distance visual acuity before surgery with the uncorrected distance visual acuity after surgery. The intraocular pressure (IOP) was measured 1 week, 1 month, and 3 months after surgery. The central vault at 3 months was measured using optical coherence tomography.
Results
Three months after surgery, the mean uncorrected distance visual acuities were −0.09 ± 0.12 logarithm of the minimal angle of resolution units with the V4b and −0.07 ± 0.11 logarithm of the minimal angle of resolution units with the V4c. The mean distances between the ICL and the anterior crystalline lens surface were 557 ± 224 μm and 528 ± 268 μm for the V4b and V4c, respectively ( P = .73). After 1 week and 1 month, the mean IOPs were 13.7 and 13.3 mm Hg and 14.7 and 15.1 mm Hg, respectively. There were no significant differences in IOP within or between groups during the follow-up period ( P > .05, for all comparisons).
Conclusions
The new ICL with the CentraFLOW design seems to provide similar results as its predecessors for the correction of moderate to high myopia and maintenance of safe IOP levels without iridotomy.
Phakic intraocular lenses (pIOLs) of different designs and materials have been developed as valuable alternatives to corneal refractive surgery. Although a number of pIOL designs and modifications have been implemented worldwide, the United States Food and Drug Administration has approved only 2 pIOLs: the anterior chamber iris-fixated Artisan/Verisyse pIOL (Ophtec BV, Groningen, The Netherlands/AMO, Santa Ana, California, USA) that was approved in 2004 and the posterior chamber Visian Implantable Collamer Lens (Visian ICL; STAAR Surgical Company, Nidau, Switzerland) that was approved in December 2005. The Visian ICL has been reported to be a valuable surgical option to treat various degrees of ametropia. Two pIOLs currently are undergoing Food and Drug Administration phase 3 clinical trials: the iris-fixated anterior chamber Veriflex/Artiflex (Ophtec BV/AMO) and the angle-supported AcrySof Cachet anterior-chamber pIOL (Alcon Laboratories, Inc, Fort Worth, Texas, USA). Recent studies have shown that the latter pIOL had an acceptable safety profile in patients with myopia. However, potential complications such as long-term endothelial cell loss are a concern. Oversizing of the pIOL can produce excessive vaulting and rapid endothelial cell loss when the internal diameter of the anterior chamber is not well correlated with the white-to-white values. Elevated intraocular pressure (IOP) is a potential adverse event associated with anterior chamber pIOLs. The Visian ICL is a posterior chamber pIOL manufactured by Staar Surgical Company and has been reported as a valuable surgical option to treat ametropia of various refractive ranges.
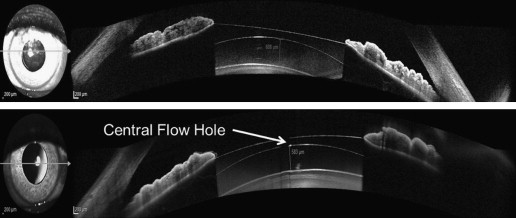
Recently, a new type of Visian ICL has been developed: the Visian ICL V4c with CentraFLOW technology. A central artificial hole called the KS-AquaPORT was added to the center of the ICL optic to improve aqueous humor circulation in the eye. This new development eliminates the need for a preoperative peripheral laser iridotomy or intraoperative peripheral iridectomy, which simplifies the surgical procedure and significantly reduces the complications associated with iridotomy such as hyphema, inflammation, or vitreous and rhegmatogenous retinal detachment. Moreover, uneventful preoperative laser iridotomy may develop a postoperative pupillary block if residual viscoelastic blocks the normal aqueous humor flow or because of closure of a previously patent iridotomy. However, it is necessary to evaluate the impact of this new surgical approach on elevations in IOP in the immediate and intermediate postoperative periods, which depend on the physical relationship between the IOL implant, the crystalline lens, and the iris, among other factors.
Earlier studies have evaluated the distance between the ICL and the crystalline lens using ultrasound biomicroscopy, Scheimpflug photography, or the first generations of spectral-domain optical coherence tomography (OCT) technology. New Spectralis OCT (Heidelberg Engineering, Heidelberg, Germany) with an anterior segment module offers image acquisition of the anterior chamber and provides high-resolution measurements of the distance between the posterior ICL surface and the anterior crystalline lens pole. This distance, referred to as vault, is the most important issue involved in ICL-induced complications, such as pupillary block and cataract formation. Ongoing concerns exist about the risk of late-onset cataract formation, presumably resulting from direct physical contact between the ICL and the crystalline lens, and disruptions in aqueous flow that interfere with lens nutrition and cause metabolic disturbances in the crystalline lens. The new Visian ICL V4c with CentraFLOW was developed to eliminate such disadvantages. The purpose of the current study was to compare the clinical outcomes with the Visian ICL V4c design with CentraFLOW technology without the need for a peripheral iridotomy with the conventional model V4b.
Methods
The study protocol was reviewed and approved by the Ethics Committee of Hospital Universitario Morales Meseguer, Murcia, Spain, and was in agreement with the standards of clinical practice and national and international guidelines. Following the tenets of the Declaration of Helsinki, patients were informed about the surgical details and provided written informed consent.
This study included 17 eyes of 9 patients implanted with the Visian ICL V4b model and 18 eyes of 10 patients implanted with the new Visian ICL V4c model at Clínica Novovisión Dr Ramón Gutiérrez, Murcia, Spain, from September 2011 through April 2012. Complete ophthalmologic examinations were performed that included manifest and cycloplegic refractions, keratometry and corneal topography with the Pentacam (Oculus Optikgeräte GmbH, Wetzlar, Germany), Goldmann applanation tonometry, and binocular indirect ophthalmoscopy through dilated pupils.
The inclusion criteria for ICL implantation were age between 20 and 45 years, a stable refractive error during the previous 18 months, and a preoperative spectacle spherical power between −3 and −15 diopters (D). The exclusion criteria included anterior chamber depth of less than 2.8 mm, a history of glaucoma or ocular inflammation, pre-existing corneal disease, and endothelial cell density of less than 2500 cells/mm.
Implantable Collamer Lens Selection and Characteristics
The one-piece ICL pIOL is made of collamer, a hydrophilic material composed of collagen and poly-hydroxyethyl methacrylate-based copolymer. The lens is available in spherical powers ranging from −3.0 to −23.0 D and astigmatic corrections of 1.0 to 6.0 D. The lens size was defined using the manufacturer calculator software according to the horizontal white-to-white distance obtained by partial coherence interferometry (IOLMaster; Carl Zeiss Meditec, Jena, Germany).
Two subsequent groups were formed with the last ICL V4b model for myopic correction and the first ICL V4c model implanted. Patients scheduled for intraocular refractive surgery from September 2011 through May 2012 were enrolled in this trial. The preoperative demographics of the study population are shown in the Table .
| Parameter | ICL V4b | ICL V4c | P Value |
|---|---|---|---|
| No. of eyes | 17 | 18 | |
| Gender | |||
| Male | 8 (47%) | 3 (17%) | |
| Female | 9 (52%) | 15 (83%) | |
| Age (y) | 32.6 ± 7.2 | 34.5 ± 9.5 | .48 |
| Range | 26 to 45 | 26 to 50 | |
| Manifest refraction (D) | |||
| Sphere | −7.95 ± 3.77 | −7.68 ± 3.7 | .938 |
| Range | −3.25 to −15.25 | −1.75 to −17.25 | |
| Cylinder | −1.51 ± 1.13 | −1.81 ± 1.33 | .578 |
| Range | 0.00 to −3.50 | −0.50 to −5.50 | |
| ACD (mm) | 3.43 ± 0.37 | 3.25 ± 0.18 | .09 |
| Range | 2.8 to 3.91 | 2.98 to 3.52 | |
| WTW (mm) | 12.15 ± 0.75 | 11.96 ± 0.4 | .68 |
| Range | 11.09 to 13.60 | 11.25 to 12.63 | |
| ICL design | |||
| ICM | 9 (53%) | 11 (61%) | |
| TICM | 8 (47%) | 7 (39%) |
Vault Assessment With Spectral-Domain Optical Coherence Tomography
A Spectralis SD-OCT (Heidelberg Engineering, Heidelberg, Germany) with the anterior segment module was used to acquire images of the anterior chamber; a detailed view of the ICL and its relationship with intraocular structures was obtained at the 3-month visit ( Figure 1 ). The same observer performed all OCT examinations and vault measurements to determine accurately the implant position in relation to the crystalline lens. OCT was performed under low light conditions, and no pharmacologic agents were used. A fixation light was used for the fellow eye to maintain a fixed amount of accommodation.
Surgical Technique
Two neodymium:yttrium–aluminum–garnet laser iridotomies were created at the 10- and 2-o’clock positions 2 weeks before surgery in the ICL V4b group. No iridotomies were performed in the ICL V4c group.
The same surgeon (R.G.-O.) performed all surgeries uneventfully under topical anesthesia (1% lidocaine). After creating a 3.2-mm clear corneal incision at the steepest meridian, the ICL was inserted with an injector (STAAR Surgical Co.) into the anterior chamber that previously was filled with sodium hyaluronate viscoelastic (Provisc; Alcon Laboratories, Inc). The footplates were placed behind the iris using a fine spatula. Viscoelastic was replaced by balanced salt solution. The wound was closed by stromal hydration after 1 mg cefuroxime sodium was injected into the anterior chamber. The postoperative therapy included topical moxifloxacin hydrochloride (Vigamox; Alcon Laboratories Inc) 4 times daily for 1 week and dexamethasone (Dexafree; Thea Laboratories, Barcelona, Spain) tapered over 5 weeks.
Postoperative examinations of the uncorrected distance visual acuity, best-corrected distance visual acuity (CDVA), manifested refraction, Goldmann applanation tonometry, and anterior chamber OCT vault were performed on day 1, week 1, and months 1 and 3. A subjective evaluation of the presence of halos and dysphotopsia was carried out by asking the patients and recorded as yes or no.
Statistical Analysis
The Snellen VA was converted to the logarithm of the minimal angle of resolution values. Statistical analysis was performed using SPSS for Windows software version 19.0 (SPSS, Inc, Chicago, Illinois, USA). Descriptive statistics were obtained. The normality of data distribution of the measured outcomes was tested using the Shapiro-Wilk test. For all statistical tests, a P value of less than .05 was considered significant. The independent samples Mann–Whitney U test was used to compare the postoperative visual function between the 2 groups. Statistical comparisons between the preoperative and postoperative IOP values in each group were carried out using a repeated measures analysis of variance with post hoc correction (Bonferroni) for multiple comparisons. The independent samples t test was used to compare the postoperative IOP values and vault readings between the groups.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


