Table 32.1 KEY POINTS IN THE DISCUSSION OF IOL IMPLANTATION WHEN THERE IS AN ABSENCE OF CAPSULAR SUPPORT | |||||
|---|---|---|---|---|---|
|
entered, and the suture is taken out with a hook. The suture is cut, and the end is tied to the eyelet of the IOL haptic. If the surgeon desires four-point fixation of the IOL, the above steps are repeated (Figs. 32.1 and 32.2). It should be noted that the main advantage of the ab externo approach is its greater precision in the location of scleral sutures.
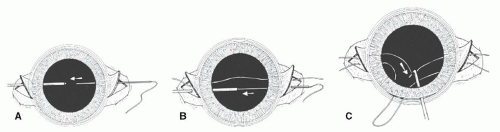 Figure 32.1. A: The double-suture variant of the Lewis ab externo technique begins similarly to the single-suture technique, except that the suture entry point under the scleral flap is displaced to one side. B: The second suture is passed parallel to the first, with 1 to 1.5 mm between the two sutures. C: Care must be taken to keep the sutures taut, to avoid crossing them or confusing which suture originates from each sclera site, while a Kuglen hook or similar instrument withdraws the suture loop through the previously prepared principal incision. (Reprinted from Steinert RF, Arkin MS. Secondary intraocular lenses. In: Stienert RF, ed. Cataract Surgery: Techniques, Complications, Management. Philadelphia, PA: Saunders, 2004:429-441, with permission.) |
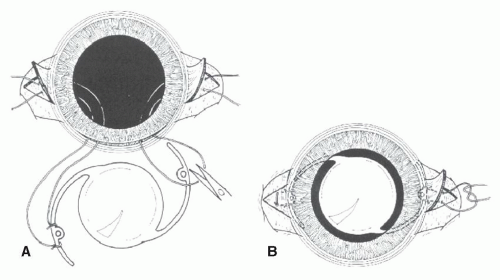 Figure 32.2. A: To achieve four-point stable fixation, the cut sutures are tied to the haptic on either side of the eyelet. B: The IOL is placed in the posterior chamber, keeping the sutures taut to avoid enlargement. The ends are then tied under the scleral flaps, and the conjunctiva is closed over the flaps. (Reprinted from Steinert RF, Arkin MS. Secondary intraocular lenses. In: Stienert RF, ed. Cataract Surgery: Techniques, Complications, Management. Philadelphia, PA: Saunders, 2004:429-441, with permission.) |
a conclusion of his Costenbader lecture, Buckley15 urged caution in the use of 10-0 polypropylene suture to fixate an IOL to the sclera in children. He recommended using an alternative material or an alternative size (9-0 polypropylene instead of 10-0). Appropriate ophthalmic needles are now available on the 9-0 Prolene suture. When necessary, however, the 9-0 Prolene suture can be tied to the end of a 10-0 Prolene and pulled through the eye using the 10-0 Prolene needle.
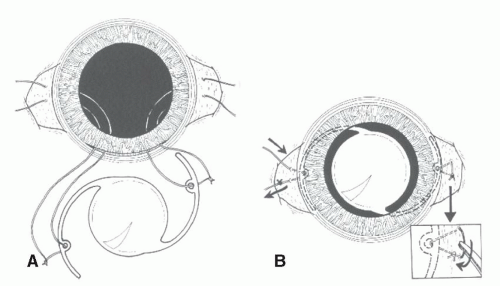 Figure 32.3. In this variant of the double-suture ab externo technique, the goal is to achieve a loop of suture where the knot can be rotated beneath the sclera, avoiding the necessity for a sclera flap. A: Cut ends of each suture are passed through the haptic positioning hole and tied. B: As the IOL is positioned in the posterior chamber, one end of the suture on each side is pulled, so it is cut off. The remaining suture ends are then tied together, and the knot is rotated beneath the sclera (inset), achieving the same result as illustrated in Figure 32.2. (Reprinted from Steinert RF, Arkin MS. Secondary intraocular lenses. In: Stienert RF, ed. Cataract Surgery: Techniques, Complications, Management. Philadelphia, PA: Saunders, 2004:429-441, with permission.) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


