Polysomnography provides information on the physiological changes occurring in many different organ systems in relation to sleep stages and wakefulness. It allows qualitative and quantitative documentation of abnormalities of sleep and wakefulness, of sleep-wake transition, and of physiological function of other organ systems that are influenced by sleep. Polysomnography is considered to be the “gold standard” for diagnosing sleep disordered breathing (SDB) and other sleep disorders; however, as with most other diagnostic tests, polysomnography is not ideal, but is rather the best available method to diagnose SDB. Review of clinical history, pre- and post study questionnaires, medications, and technician’s comments at the time of interpreting the PSG provides a unique opportunity to correlate clinical and electrophysiological data, and is a good investment of time toward improving patient outcomes and avoidance of unnecessary testing.
The term “polysomnography” (PSG) has Greek and Roman roots, and refers to the recording of multiple sleep-related signals. It employs various methods to simultaneously and continuously record neurophysiological, cardiopulmonary, and other physiological parameters over the course of several hours, usually during an entire night (overnight polysomnography). PSG provides information on the physiological changes occurring in many different organ systems in relation to sleep stages and wakefulness. It allows qualitative and quantitative documentation of abnormalities of sleep and wakefulness, sleep-wake transition, and of physiological function of other organ systems that are influenced by sleep. Many of these, such as sleep apnea, may not be present during wakefulness.
Four types of sleep studies are available, depending upon the number of physiological variables recorded :
Level I. Standard PSG with a minimum of seven parameters measured, including electroencephalogram (EEG), electro-oculogram (EOG), chin electromyogram (EMG), and EKG, as well as monitors for airflow, respiratory effort, and oxygen saturation. A technician is in constant attendance.
Level II. Comprehensive portable PSG studies are essentially the same, except that a heart rate monitor can replace the ECG and a technician is not in constant attendance.
Level III. Modified portable sleep apnea testing is a cardiorespiratory study in which a minimum of four parameters must be measured, including ventilation (at least two channels of respiratory movement, or respiratory movement and airflow), heart rate or EKG, and oxygen saturation. Ventilation in this case is measured with at least two channels of respiratory movement or of airflow. Personnel are needed for preparation, but the ability to intervene is not required for all studies.
Level IV. Continuous (single or dual) bioparameter recordings where devices that measure a minimum of one parameter, usually oxygen saturation are utilized.
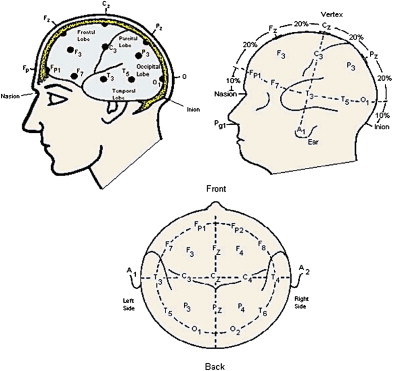
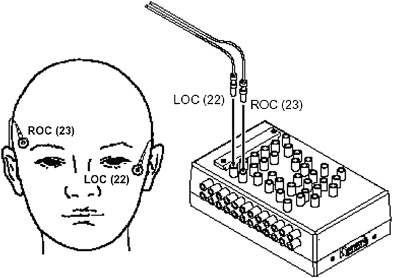
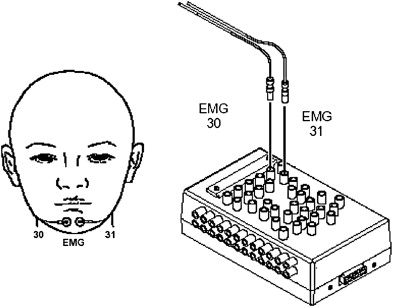
This article focuses on interpretation of Level I studies (attended PSG). According to the recently revised criteria published by the American Academy of Sleep Medicine (AASM), the following parameters should be recorded: Electroencephalogram (EEG) derivations (frontal, central and occipital) ( Fig. 1 ), bilateral Electrooculogram (EOG) ( Fig. 2 ), Chin electromyogram (EMG) ( Fig. 3 ), leg EMG, airflow, respiratory effort, oxygen saturation and body position . EKG is recorded routinely during all PSG studies. Video monitoring during a PSG, although not required, is extremely valuable, both from a diagnostic as well as medico-legal perspective.
Additional variables can be recorded according to patient age, standards of the sleep laboratory, and indication for performing the study. Examples of such additional variables include end-tidal carbon dioxide monitoring (EtCO2), 16-channel EEG recording for seizures, esophageal pressure monitoring (Pes), and pulse transit time (PTT). AASM [formerly The American Sleep Disorders Association (ASDA)] recommends performing at least 6 hours of overnight recording . The neurophysiological, EKG, and sound channels are sampled at 100 to 1000 Hz with 12- to 20-bit resolution, respiratory mechanical channels at 50 Hz, and pulse oximetry and body position, at a significantly lower rate. The modern day computerized PSG systems provide powerful tools for technicians and physicians to customize data acquisition. One can change reference electrodes, resolution, and sensitivity, and add or remove digital filters to minimize recording artifacts. Many of these functions can be performed even after the data have been acquired, which allows interpretation of the studies despite malfunction of certain equipment during the recording.
EEG is the recording of surface electrical activity of the brain. Only limited EEG data are obtained during a PSG recording to help identify stages of sleep and wakefulness. EOG is the recording of eye movements during sleep and wakefulness. The cornea and retina form a dipole, with the cornea being negative in relation to the retina. A movement in the eyes changes the electrical signal in the EOG electrodes, which is recorded as a deflection. The EOG electrodes are placed slightly outside the outer canthus of each eye, with one electrode being slightly lower than the other (see Fig. 2 ). This enables detection of horizontal as well as vertical movements of the eyes. EEG, EOG, and submental EMG are essential for sleep staging. Submental and leg (tibialis anterior) EMG recordings are performed routinely during PSG. The submental EMG recordings are essential for scoring sleep stages, especially rapid eye movement (REM) sleep. Three electrodes are placed for submental EMG recordings, in order to have a backup in case one of them malfunctions during the sleep study (see Fig. 3 ). Typically, the submental EMG tone is lowest during REM sleep. It is also helpful in detecting sleep bruxism (see below). Bilateral leg EMG recordings are used to diagnose periodic limb movements of sleep (PLMS). Additional EMG recordings can be used under special circumstances. For example, both upper and lower extremity EMG can be recorded for suspected REM behavior disorder (RBD), and gastrocnemius muscle EMG could be recorded for diagnosing nocturnal leg cramps. Snoring is recorded with a microphone, and airflow is measured with the help of a thermistor or with a nasal pressure monitor. The thermistor measures changes in the electrical conductance in response to temperature changes in the probe, which occur with inspiration and expiration. Continuous recording of body position by an accelerometer is important, because snoring and upper airway obstruction during sleep are influenced by gravity . The most common indication for performing a PSG is diagnosis of sleep disordered breathing (SDB) and its treatment with positive airway pressure (PAP). Other indications for PSG include: evaluation for effectiveness of alternative treatments for SDB (eg, dental appliances or surgical procedures, diagnosis of sleep-related seizures, parasomnias, and evaluation of erectile dysfunction with nocturnal penile tumescence [NPT]).
Important considerations
Polysomnography is considered to be the “gold standard” for diagnosing SDB and other sleep disorders. A gold standard should have 100% sensitivity and specificity ; however, like most other diagnostic tests, PSG is not ideal, but rather the best available method to diagnose SDB. Furthermore, breathing disturbances may vary from night to night within certain limits . Some sleep disorders such as nocturnal laryngospasm, sleep-related epilepsy, or parasomnias that occur episodically may be missed in a one-night recording .
A PSG should always be interpreted in light of a patient’s clinical history. The physician’s orders should be reviewed to determine the reason for obtaining the PSG and for the type of study requested. The interpreting physician should ascertain that the PSG was performed as requested. If a split-night study (diagnostic and PAP titration in the same night) was ordered but the patient has difficulty sleeping, demonstrates only mild obstructive sleep apnea (OSA), or does not tolerate the PAP trial, it is helpful to write a brief explanation as to why PSG was not performed as requested. This helps the referring physician to decide whether to order another study with PAP trial, or to refer the patient for alternative therapies.
It is pertinent to review the referring physician’s notes and the prestudy questionnaire before interpreting PSG. The referring physician’s notes provide information on comorbid conditions that may increase the likelihood of prevalence of certain sleep disorders. For example, heart failure with ejection fraction of less than 40% increases the risk of having Cheyne-Stokes breathing, hypothyroidism increases the likelihood of having OSA, and Parkinson’s disease is associated with higher incidence of RBD. The physician’s notes are also helpful in explaining certain findings on the PSG, such as cardiac arrhythmias or abnormal oxygen saturation at baseline.
Generally, each patient is given a pre-study questionnaire to fill out before performing the PSG. This questionnaire provides sleep history in greater detail than is usually available otherwise. The questionnaire is intended to obtain information on patient’s sleep-wake schedule and various sleep symptoms such as snoring, excessive daytime sleepiness, witnessed apneas, irresistible urge to move legs, dream enactment, teeth grinding, cataplexy, and so forth. The patient’s usual bedtime and rise time are taken into account when commenting on sleep latency and efficiency (see below). Some degree of insomnia can be expected in the unfamiliar environment of the sleep laboratory, especially on the first night (first-night effect) .
Most questionnaires also incorporate the Epworth Sleepiness Scale (ESS) . ESS has eight questions about subjective sleepiness under routine activities, and the patient answers them on a scale of 0 to 3, the highest possible score being 24 ( Appendix, Table 1 ). A score of 12 or more is indicative of excessive daytime sleepiness, whereas a score of 10 to 12 is considered borderline. It should be noted that many patients who have SDB and low ESS score may show hypersomnia on objective measures such as the Multiple Sleep Latency Test (MSLT) . The patient is also asked about any sedatives taken before the PSG. The authors do not administer, nor do we recommend administering, any medications (other than patient’s usual regimen) for the purpose of promoting sleep during PSG recording. Most patients are able to sleep for sufficient duration in the sleep laboratory to allow acquisition of interpretable data.
Because most sleep centers do not have nurses at night, dispensing the medications and assessment of patients before discharge after the study may compromise patient safety if medications are administered for the sleep study. Sedatives have unpredictable side effects, and may impair the patient’s driving ability the next morning. They also skew the sleep architecture, can potentially worsen obstructive sleep apnea or attenuate central sleep apnea, RBD, and PLMS, thus interfering with the diagnosis. Other medications, which could affect sleep, should also be noted. For example, many antidepressants suppress REM sleep and increase EMG tone during REM sleep.
The importance of technician comments cannot be overemphasized, because they provide an excellent source of additional information. The technician should fill out a checklist, which includes information about nocturnal oxygen usage, sedative, and alcohol usage among other things. The technician also makes notes of additional monitoring performed during the study (EtCO2, Pes) so that the reviewing physician can modify the montage when analyzing PSG data. Any technical difficulties encountered during the recording and any specific problems encountered by the patient, such as pain, panic, or breathing difficulty, that could be corroborated with the PSG findings are also mentioned. If a PAP titration is performed, the technician makes note of types of interfaces tried, interface with the best fit, patient preference for a specific interface, mouth breathing, use of humidifier, chinstrap, and use of bi-level PAP. Each time a change is made in PAP setting, the technician cites the reason for this. All this information should be taken into account for correct interpretation of a PSG.
Last but not the least, a post-study questionnaire completed by the patient after the PSG provides an important insight into the patient’s overall experience. If PAP titration was performed, it is important to note the patient’s attitude toward PAP therapy. Specific problems reported by the patient during PAP titration (eg, nasal congestion, claustrophobia or pressure intolerance), can be specifically targeted and the treatment tailored to individual needs of the patient.
Video recording
The authors routinely perform video recording on all patients coming to our sleep laboratories, and a written consent for this is obtained from every patient. Video recording should begin from the time of starting the hookup, and should continue until the study is completed. It provides objective assessment of seizures, sleep-related movement disorders, and parasomnias. It can also be used to confirm the patient’s position in case of doubt. It may sometimes be possible to see mouth opening and paradoxical respiratory movements on the video. Video also provides added security to the patient and the laboratory personnel from inappropriate interaction or allegations of such an interaction. The video files typically consume a large amount of storage space. DVD and tape drives are the currently preferred methods of storing video data.
Video recording
The authors routinely perform video recording on all patients coming to our sleep laboratories, and a written consent for this is obtained from every patient. Video recording should begin from the time of starting the hookup, and should continue until the study is completed. It provides objective assessment of seizures, sleep-related movement disorders, and parasomnias. It can also be used to confirm the patient’s position in case of doubt. It may sometimes be possible to see mouth opening and paradoxical respiratory movements on the video. Video also provides added security to the patient and the laboratory personnel from inappropriate interaction or allegations of such an interaction. The video files typically consume a large amount of storage space. DVD and tape drives are the currently preferred methods of storing video data.
Electroencephalography and electro-olfactography
A standard 10 to 20 EEG electrode placement system is used in placing the electrodes for recording of sleep (see Fig. 1 ). The recommended standard derivations for EEG recording are F4-M1, C4-M1, O2-M1. The EOG electrodes (ROC and LOC) are placed as shown in Fig. 2 . Mastoid (auricular) electrodes are used as references. Conventionally right-sided electrodes are assigned even numbers (C4, O2) and left sided electrodes are assigned an odd number (C3, O1). The EEG electrodes could be referenced to mastoid electrodes (M1 and M2 [A1 and A2 in older terminology]) (see Fig. 1 ) or to a common reference electrode. Typically right-sided electrodes (O2, C4 and ROC) are referenced to left mastoid (M1) electrode and left sided electrodes (O1, C3 and LOC) are referenced to right sided electrodes (M2). The drawback of using mastoid electrodes is that EKG artifact commonly appears in these electrodes making it difficult to staging sleep in some old systems ( Fig. 4 ). With the older systems, placing the auricular electrodes higher, jumping the two auricular electrode, or using a common reference electrode can minimize EKG artifact. The newer PSG systems use software to filter EKG artifact.
Before reviewing digital PSG, it is important to ensure proper setting of the desktop display for resolution. It is recommended that the monitor for reviewing PSG should have a resolution of at least 1280 × 1024 and be 20 inches or larger for proper identification of waveforms and sleep staging and video reviewing . The digital systems allow creation, storage, and individual configuration of several different montages for different users. One can adjust the sensitivity, trend color, and display range among many other variables. The display range is usually between 10 to 480 seconds. Sleep is usually staged according to the Rechtschaffen and Kales criteria in 30-second epochs . In case of difficulty, reducing the display range to 10 seconds is helpful in recognition of EEG waveforms. On the other hand, detection of certain respiratory patterns is better appreciated by compressing the waveforms obtained over 60 to 480 seconds on the screen ( Fig. 5 ).
Another important consideration is checking the biocalibration data. Before the actual sleep recording is started, the technicians ask patients to perform certain voluntary maneuvers such as closing and opening of the eyes, moving the eyes vertically and horizontally, moving the legs, clenching the teeth, rapid breathing, and breath holding. This is useful in ensuring that all the electrodes are functioning and are recording the signal as intended. These waveforms serve an important reference for comparison later during the sleep study. The technicians also check and document impedance in the beginning and periodically during the study, to ensure accuracy of the recorded parameters.
Sleep staging
Until recently sleep staging was based on the original Rechtschaffen and Kales’ criteria devised more than 30 years ago. The AASM task force has recommended implementation of new criteria for sleep staging, which will replace the current staging system [2]. Sleep is now scored in the following stages; stage awake (W), NREM stages 1, 2, 3 ( N1, N2 and N3 respectively) and stage REM (R) sleep. EEG, EOG and chin EMG are required to score the sleep stages. The identification of EEG waveforms is helpful in scoring sleep. The central leads (C4 and C3) are most helpful in the identification of EEG waveforms, except alpha waves, which are most prominent in the occipital leads.
There are four different waveforms based upon the frequency of the rhythm, alpha waves are fast frequency (8–12 Hz) ( Fig. 6 ). Beta waves ( Fig. 7 ) consists of fast frequency of greater than 13 Hz. They are most prominent during stage awake and eyes open. They are of low amplitude and disappear during sleep. The frequency for theta waves ranges from 4–8 Hz ( Fig. 8 ) and for delta waves it is less than 4 Hz ( Fig. 9 ). Theta frequency is the most prevalent frequency seen during a polysomnography. In addition to these four frequencies, four morphologic waveforms are important. Vertex waves are sharp negative waves (in EEG terminology, a negative wave causes an upward deflection ) ( Fig. 10 ). They first appear in stage N1 sleep and are most abundant during stage N2 sleep. K-complex is a biphasic wave with an initial upward (negative) deflection followed by a slower downward (positive) deflection (see Fig. 8 ). Sleep spindles are so-named because of their characteristic shape. They have a frequency of 12 to 14 Hz and duration of 0.5 to 1.5 seconds ( Fig. 11 ). K-complexes and sleep spindles are characteristic of stage 2 sleep. Sawtooth waves also have a characteristic appearance ( Fig. 12 ). They have low amplitude and are in the theta frequency.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


