3
Internet-Based Self-Help Treatment of Tinnitus
This chapter presents a novel approach to tinnitus management with a cognitive-behavioral treatment protocol implemented via the Internet. Self-help in the management of tinnitus is reviewed, as well as practical aspects of the protocol. These include adherence, security, and technical problems. Effects of the protocol are briefly mentioned.
Background
Self-Help Material for Tinnitus
The self-help books industry is a growing market, and many people with debilitating conditions never seek professional help. It is therefore not surprising that people attempt to treat themselves without the involvement of health care professionals and hospital facilities. In addition, many people read self-help books at the same time as they are in treatment. This can be a recommendation from the therapist or resulting from pure interest. A survey of practicing psychotherapists revealed that over 80% were recommending self-help resources to their clients (Norcross et al, 2000). In addition, self-administrated treatments do rarely result in any negative outcome (2–3%), at least not more than in regular treatment (Scogin et al, 1996). For all parts involved, cost effectiveness is an important aspect of the health service provided. Away to reduce the costs is therefore to minimize contact with the therapist and to let patients treat themselves, supported by books and structured self-help manuals. Tinnitus is a good example of a prevalent condition where the need for self-help is great. First, many tinnitus patients never get to see a professional tinnitus clinician. Second, only a few patients need to go through an extensive therapy program, and many benefit from learning more about their condition and how to deal with it on their own.
For many conditions such as headache, sleep problems, and anxiety there is empirical support for the use of self-help materials (often referred to as bibliotherapy). Self-help books can be a good alternative when professional therapy is inaccessible or considered too expensive. Although numerous books exist on the market only a fraction of these have been tested in empirical studies (Norcross et al, 2000). A list of commonly used and researched self-help books, relevant for the tinnitus clinician, is presented in Table 3–1.
Usually, studies of socalled self-help treatments have included some form of contact with the therapist; for example, by means of telephone calls. Hence a more proper name is minimal therapist contact treatment. Although many tinnitus sufferers seek help outside of health care settings (e.g., the Internet), clinicians have paid little attention to the idea of alleviating tinnitus via self-help material. However, self-help groups are often set up, and years of experience confirm their usefulness (Reich, 2000).
In many countries, information brochures on tinnitus are available. These are often issued by national societies, as, for example, by the Swedish Hard of Hearing Association, the American Tinnitus Association, and the Royal National Institute for Deaf People. Alternatively, folders are produced and distributed by local clinics in the form of photocopied handouts.
Several books have been published on tinnitus, and some have been aimed at a broader audience than researchers and clinicians. Moreover, the national tinnitus organizations have been instrumental in spreading information regarding tinnitus and its treatment. It is beyond the scope of this chapter to review all of the abundant literature and information on tinnitus, so we will comment on just a few examples.
Regarding psychological management of treatment, an influential book was published in 1989 by the psychologist Richard Hallam (Hallam, 1989). This book has been translated into at least two other languages (Swedish and German) and includes good advice. Most of its content is still relevant today, but perhaps the section on masking therapy has been outdated by the passage of time and the recent development of our understanding of masking as a treatment for tinnitus. Davis (1995) published a self-help book, Living with Tinnitus, that includes good advice. The format of this book makes it highly accessible to most patients and a good start for those who want to learn more about the condition. More recently, Henry and Wilson (2002) published a self-help book, Tinnitus: A Self-Management Guide for the Ringing in Your Ears, in which their cognitive-behavioral treatment approach is made accessible in the self-help format. There are also books available that contain more specialized information, basically reviewing research (e.g., Vernon, 1998). Among these are Sheppard and Hawkridge’s Tinnitus: Learning to Live with It (1987). Finally, we have more advanced material in the form of books for professionals (e.g., Tyler, 2000). We all know that many patients are well educated and have no problem following the scientific literature. Nonetheless, some choose not to, and of course there are plenty of patients for whom it is impossible to grasp the scientific literature.
| Condition | Book |
|---|---|
| Depression | Burns, DD Feeling good: The New Mood Therapy: Revised and Updated. New York: Avon; 1999 |
| Insomnia | Hauri P, Linde S. No more sleepless nights, rev. ed. New York: John Wiley and Sons; 1996 |
| Panic disorder | Zuercher-White E. An End to Panic: Breakthrough Techniques for Overcoming Panic Disorder. 2nd ed. Oakland, CA: New Harbinger; 1998 |
| Anxiety overall | Bourne EJ. The Anxiety and Phobia Workbook. 3rd ed. Oakland, CA: New Harbinger; 2000 |
It is clear that information on tinnitus is abundant. However, from the scientific literature we know that self-help on its own rarely is effective, and that some form of guidance, however small, must be provided. In this chapter we will describe our experiences with a self-help program for tinnitus, and in particular we will focus on how self-help can be implemented via the Internet.
Self-Help Material for Tinnitus on the Internet
The Internet has dramatically changed access to information and the spread of such information worldwide. It has become a regular part of many people’s lives, including in the use of the Internet in seeking health care advice and assistance. In fact, health care information is said to be one of the most retrieved types of information on the World Wide Web (Eysenbach et al, 1999). As the amount of medical information on the Internet has grown rapidly, concerns have been raised that the material needs to be filtered (Eysenbach and Diepgen, 1998), and that some form of quality control is needed. For example, patients often turn to the Internet to confirm diagnoses, validate clinician-recommended treatment, and seek alternative therapies (Bader and Braude, 1998). In addition, clinicians use the Internet to communicate with their patients (Kuppersmith, 1999), a practice to which there are advantages as well as potential problems. Moreover, through telemedicine, several interesting applications of the Internet have been developed (Mair and Whitten, 2000).
The Internet revolution has led to the production of several Web pages dealing with tinnitus. Although important information can be accessed that way, there is no quality control (Eysenbach and Diepgen, 1998), and it is easy to be misled.
Internet-Based Self-Help
One potential way to provide self-help material in a structured manner is via the Internet. Providing treatment via the Internet has advantages over self-help books in that advice can be given on an ongoing basis without delay. In comparison with ordinary treatment, Internet-based self-help treatment can be cost effective; it also makes the treatment available to people living far from the specialist’s practice.
We have developed a clinical program in which self-help is investigated for various conditions (e.g., Carlbring et al, 2001; Ström et al, 2000), including tinnitus (Andersson et al, 2002; Kaldo et al, 2004). The approach involves therapist interaction either via e-mail or supplemented with telephone calls, and all treatment is based on cognitive-behavioral principles. The main difference from previous self-help studies is that in Internet-based self-help treatment, all material is provided via Web pages. As we will return to later in this chapter, we have also developed a tinnitus treatment, largely based on the protocol described in Chapter 8. This is the program we have had the most clinical experience with in our audiology clinic in Uppsala, Sweden.
Necessary Background and Facilities
All patients need to have access to computer, modem, and Internet connections, and should be able to print out the training instructions. The intention is to make the treatment instructions easily available (technically easy), and computer experience is probed during the structured interview. However, some people may have access to a computer but not one of their own. Because privacy may be an important factor, this issue should be discussed with the patient. In the treatment rationale, the role of the Internet actually needs to be deemphasized because the content of the treatment could very well be presented in a book. However, the interactive part of the Internet should be put forward as an advantage. We require that patients go through a proper medical and audiological screening before they start treatment. The Web pages are not “open,” and are accessible only with a password, given by e-mail to the patient. In cases when the Internet fails to work, or when patients have problems with their connection, the possibility to contact us over the phone is given. It is perfectly possible to go through all the steps without any personal contact, but in clinical practice we see the patient for a first assessment session, and preferably for a follow-up. However, all registration forms and rating scales have been converted into Web pages and are filled out via the Internet.
The Protocol
As mentioned, the Internet self-help treatment is basically a translation of our regular treatment protocol but with certain alterations due to the format. The first open pages include information about tinnitus (see Table 3–2), what is required to follow the program, an overview of the treatment program, and a special page for referring authorities. Then, links to the assessment page and treatment pages are given. These require passwords, which we mail to the patients. Internet treatment should not be seen as a substitute, but rather as a complement to tinnitus management at the home clinic. However, because few psychologists are involved in tinnitus rehabilitation (Coles, 1992), self-help represents a promising alternative in combination with other forms of management.
| Definition of tinnitus |
| What we know about tinnitus |
| Prevalence |
| Causes and related factors |
| More on hearing impairment |
| Other causes and related factors |
| Meniere’s disease |
| Hyperacusis |
| Otosclerosis |
| Tinnitus and normal hearing |
| Tinnitus and psychology |

Figure 3–1 First procedures for entry into cognitive behavioral treatment (CBT) via the Internet.
The whole process from referral to completed treatment is outlined in Figs. 3–1, 3–2, and 3–3. In our clinic we conduct a structured interview with each patient before Internet treatment is started.
HOW TO FOSTER ADHERENCE
The implementation of the Uppsala treatment program via the Internet has been possible without any major revisions. However, certain practical aspects must be detailed to avoid misunderstanding the purpose of Internet-based self-help treatment of tinnitus. Self-help treatment is not a quick fix, and it does not consist only of information. Patients should be aware of the fact that they need to devote at least 30 to 45 minutes per day to the treatment exercises. In order for the program to have any effect, it is crucial that the patients go through the exercises and that they e-mail us if there are any questions or technical problems. The program is set up in six modules that basically mirror our face-to-face treatment. All modules involve homework assignments and reports on a Web page to be submitted weekly. Patients are encouraged to ask questions regarding the treatment, and all queries are answered as promptly as possible by the therapist or the physician. When submitting a weekly report, the patient is sent an e-mail with feedback on treatment progress, focusing on the positive aspects. Moreover, misconceptions about immediate treatment effects and (for some patients) a desire to adhere too strictly to the instructions given are sorted out. For example, patients may believe that the treatment will not be of any help if they are unable to practice as many times as instructed. Another use of e-mail feedback is to help patients go through the treatment within a reasonable amount of time. Some may need to be encouraged to fill in the diary and to move on to the next module. The code for each consecutive module is given automatically.
THE MODULES
A rationale is presented for each component of the treatment. In this section we will comment on the treatment modules as they are presented on the Web pages.
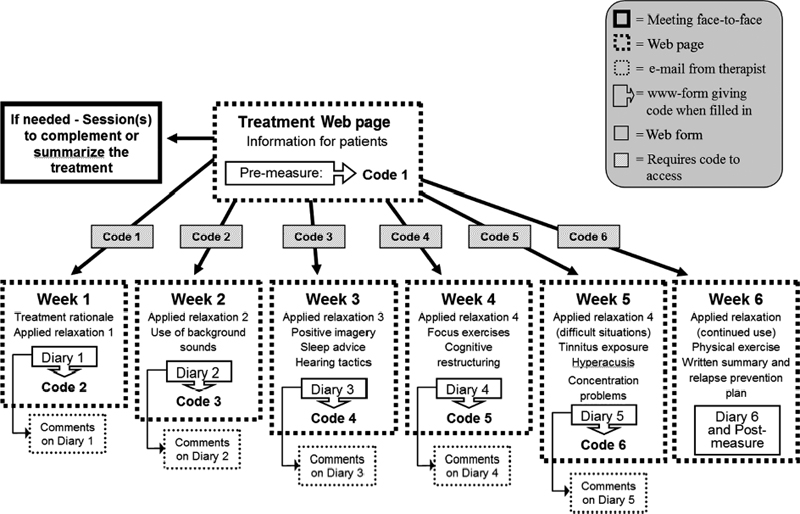
Figure 3–2 Treatment Web pages for 6 weeks.

Figure 3–3 Follow-up procedures.
First Week A treatment rationale is presented, including psychological mechanisms and how they may affect tinnitus (see Chapter 8). An example of a vicious cycle is given (see Fig. 3–4). Applied relaxation step 1, Progressive relaxation (tense and release body parts), is presented in the text version. A potential disadvantage of Internet-administrated relaxation training is that we have no way to observe if the relaxing is practiced properly. Hence, homework compliance and weekly report cards of progress are very important to monitor patients’ progress and to encourage them to send in any questions they may have. Potential problems with relaxation are covered.
Second Week Information and instructions are given regarding the next topic, “Tinnitus and environmental sounds and use of environmental sound enrichment strategies for facilitation of habituation to tinnitus.” In this text we describe the purpose of using sounds to deal with tinnitus. Also presented are tips regarding which sounds to be used. In this information the role of sudden changes, or contrasts, is explained, and it is suggested that sudden changes in background sound (e.g., from music to silence) are likely to increase the salience of tinnitus. However, although annoying, this contrast effect is not dangerous and is not a sign that tinnitus loudness has increased permanently. Regarding which sounds to use, the most important thing is that they should not be too loud. They may vary in terms of attention-grabbing properties (interest). For example, often a meaningless background sound (e.g., traffic from the street) is good when the patient is concentrating on other things, but there are also situations for which an interesting sound (e.g., a radio program) is preferable. Applied relaxation step 2, Release-only relaxation without tension, is presented in text. Release-only relaxation is given as homework for the next week (2 times per day). Registration of the use of environmental sounds is also given as homework.
Figure 3–4 Example of vicious cycle.
Third Week Applied relaxation step 3, Cue-controlled relaxation (controlled breathing), is presented. Because the Internet administration allows a flexible approach to what information to present, the patient can easily be given information about possible obstacles and problems when practicing relaxation. Instruction on how to use imagery techniques (i.e., positive imagery) is included in association with the relaxation. Also provided is advice regarding insomnia and suggestions for homework regarding sleep (Morin, 1996). Hearing tactics (Andersson, 2000) are not only for the individual with hearing problems but also directed to the people close to the patient.
Fourth Week Applied relaxation step 4, Rapid relaxation in everyday situations, is introduced, and the patient is encouraged to establish rapid relaxation as a habit. Common for all the steps in applied relaxation is that the Internet administration has been unproblematic. In other words, patients find it fairly easy to learn relaxation via the Internet. Information on attention-shifting techniques is included. For example, patients are given exercises on how to shift attention from tinnitus to other sounds, or from tinnitus to other bodily sensations or positive images. The cognitive therapy part of our self-help program begins by presenting a repetition of the treatment rationale and by explaining the “situation-cognition-emotion” perspective of understanding tinnitus distress. Also introduced are common cognitive “errors” (e.g., overgeneralization) and ways to find alternatives to negative automatic thoughts (see Henry and Wilson, 2002). Being a text-based self-help approach, this demands that the information is clear and that patients can reach us via e-mail to sort out questions and misunderstandings.
Fifth Week Repetition of the relaxation exercise (step 4) and application in different situations are encouraged on the basis of self-report of practice and use. Information on hyperacusis is presented, with a report card included. Techniques such as reinterpretation of tinnitus and gradual exposure to tinnitus/quiet environments are presented. We also give advice on how to minimize concentration difficulties. This includes structure of encoding and ways to facilitate retrieval from memory.
Sixth Week Apart from the relaxation training, this last module includes planning of when to use the exercises in the future. Another aspect of the treatment that is highly suitable for Internet use is the prevention of lapses (see Henry and Wilson, 2002). Regular physical exercise is seen as a protective factor for preventing relapse. Questionnaires for follow-up assessments are administered. In addition, after the treatment, the Web pages are available for patients as an extra way to prevent relapse.
Special Considerations
Obviously, self-help via the Internet cannot be equated with ordinary treatment at a clinic, and it is not suitable for all people. There are also other, more subtle matters to consider when implementing Internet-based treatment. One example is the role of simultaneous treatments that may have a totally different rationale. In general, we rarely regard this as a problem, but one plausible reason may be that our Internet treatment is regarded as something less real than seeing a therapist at an office. Interestingly, when we have studied this question empirically using the treatment credibility questionnaire (Borkovec and Nau, 1972), we have found no differences in perceived credibility between our ordinary treatments (group or individual) and Internet treatment.
Critics may question whether cognitive therapy really can be given over the Internet. There is empirical evidence that suggests that cognitive therapy in the form of self-help books has beneficial effects on several conditions (Norcross et al, 2000). We see no reason why Internet administration should be less effective.
What might be critical from a research point of view are placebo effects. It may be that we convey a sense of being cared for (access to contact on a continuous basis), and that patient expectations are nurtured and enhanced by the medium. There is indeed something special with the Internet, and we have seen this in several of our studies. However, the attraction of the Internet can also lead to its misuse in that the “surfer” is tempted to go and check the latest news instead of doing relaxation training. There have been reports on pathological Internet use (Griffiths, 1998), but so far we have not seen this in our clinic.
The Internet brings with it numerous possibilities. For example, in the clinic we have built-in reminders for the clinician when it is time to contact the patient; such reminders are being developed for our self-help Web pages. Also, rating scales for each of the therapy components are being developed that are more detailed. By making the homepage more interactive, we also hope to increase patient participation by letting patients plan and tailor their treatment to a greater extent.
Potential Problems and Evaluation of Effects
DISINHIBITION AND THE INTERNET
A tendency for Internet users to be disinhibited has been observed (Joinson, 1998), and it may be that it is easier to send an e-mail than it is to seek treatment via traditional routes. Moreover, it has been suggested that Internet-mediated communication is less inhibited by social norms and that this can result in misunderstandings. One suggested reason for this is that Internet communication (i.e., e-mail) lacks many of the emotional cues provided by spoken language, while still being a “rapid” form of communication without the time to reflect upon answers and comments given. However, in our clinical practice we have not yet experienced this as a problem, and it is important to remember that Internet-based treatment does not preclude telephone contact or correspondence by letter either. Also, although the Internet certainly encourages rapid responses, the practicing clinician does have the possibility to reflect and even consult colleagues before responding to the patients’ questions.
DROPOUTS OR SLOW RESPONDERS?
Perhaps because of the nature of the Internet, and because of selective recruitment in our first controlled trial, we had problems with what we first thought were dropouts from the treatment. Later this turned out to be problems caused by lack of time. In the clinic it will be immediately apparent if patients decline treatment because of time constraints. Interestingly, when implementing the Internet-based treatment in clinical practice, we have found a higher adherence to the treatment by those patients who have been referred from counties outside of our own. Most likely this is explained by their efforts in getting a referral from their home counties (which often is restricted). Compliance to Internet-based treatments is an area for future research.
SECURITY AND TECHNICAL PROBLEMS
As the Internet is increasingly used and technology is improved, issues regarding security become less difficult to solve. However, for now there is no guarantee for protection against intrusion. Rarely, if ever, is this mentioned as a problem by our patients. However, security matters should be discussed with patients, particularly if they share a computer (or an e-mail account) with family members. Clearly, problems need not arise if this is discussed before treatment. For example, personal feedback can be sent via regular mail, or the patient and the therapist can agree to leave out certain sensitive matters when corresponding via e-mail, and instead discuss them over the phone or in session.
Because we see all of our patients in a first assessment session, the risk of faked responses is decreased in comparison with our controlled trial in which participants could remain anonymous. However, unrealistic responses on questionnaires and noncompliance (while still sending in homework assignments) cannot be detected in a reliable manner. This problem also pertains to paper-and-pencil evaluations.
SOLICITED AND UNSOLICITED E-MAIL CORRESPONDENCE
E-mail is often used to send in questions to professionals (Kuppersmith, 1999). Each clinician runs the risk of being overloaded with both solicited (from patients in treatment) and unsolicited (from patients not in treatment) e-mails. Eysenbach and Diepgen (1999) did a study of 209 unsolicited e-mails mostly sent to physicians by individuals seeking advice for dermatological problems. They found that 81% of correspondents had a chronic disease and sought a second opinion. Moreover, the researchers found that 40% of all e-mails could have been answered by a librarian, 28% of all e-mails were judged to be suitable to be answered by a physician via e-mail alone, and in 27% any kind of consultation would not have been possible without seeing the patient. They concluded that e-mails could substitute a physician visit or telephone call in some cases, but that some major problems need to be solved beforehand.
In clinical practice, we need to focus on the patients who are in treatment and be careful when responding to unsolicited e-mails.
Conclusion
Access to the Internet is increasing, and many people use it to access health-related information. It is also becoming an accepted medium for clinician–patient interaction. The Internet is widely used by tinnitus patients to access information regarding their condition, as attested by the numerous Web pages dealing with the condition.
Most likely, the Internet will change the way health care is provided in the future; hence, there is an urgent need to evaluate the pros and cons of Internet-based treatment. Given the novelty of the medium, there are several issues that evolve when conducting treatment via the Internet, such as ways of recruitment, participant characteristics, and online behavior, that may differ from in-session treatments.
It is necessary to develop and test self-help approaches for the management of tinnitus. The vast majority of Web sites and self-help books have not been evaluated empirically, and it is very likely that much self-help material can be used as an adjunct to the care provided at the clinic. The Internet is promising in its capacity to reach many people at a long distance and at a low cost.
References
Andersson G. Hearing impairment. In: Radnitz C, ed. Cognitive-Behavioral Interventions for Persons with Disabilities. Northvale, NJ: Jason Aronson; 2000:183–204
Andersson G, Strömgren T, Ström L, Lyttkens L. Randomised controlled trial of Internet based cognitive behavior therapy for distress associated with tinnitus. Psychosom Med 2002;64:810–816
Bader SA, Braude RM. “Patient informatics”: creating new partnerships in medical decision making. Acad Med 1998;73:408–411
Borkovec TD, Nau SD. Credibility of analogue therapy rationales. J Behav Ther Exp Psychiatry 1972;3:257–260
Carlbring P, Westling BE, Ljungstrand P, Ekselius L, Andersson G. Treatment of panic disorder via the Internet: a randomized trial of a self-help program. Behav Ther 2001;32:751–764
Coles RRA. A survey of tinnitus management in national health service hospitals. Clin Otolaryngol 1992;17:313–316
Davis P. Living with Tinnitus. Woollahra, Australia: Gore & Osment; 1995
Eysenbach G, Diepgen TL. Towards quality management of medical information on the Internet: evaluation, labelling, and filtering of information. BMJ 1998;317:1496–1502
Eysenbach G, Diepgen TL. Patients looking for information on the Internet and seeking teleadvice. Arch Dermatol 1999;135:151–156
Eysenbach G, Diepgen TL. Towards quality management of medical information on the internet: evaluation, labelling, and filtering of information. BMJ 1998;317:1496–1502
Griffiths M. Internet addiction: does it really exist? In: Gackenbach J, ed. Psychology and the Internet. Intrapersonal, Interpersonal and Transpersonal Implications. San Diego: Academic Press; 1998:61–75
Hallam RS. Living with Tinnitus: Dealing with the Ringing in Your Ears. Wellingborough, UK: Thorsons; 1989
Henry JL, Wilson PH. Tinnitus: A Self-Management Guide for the Ringing in Your Ears. Boston: Allyn & Bacon; 2002
Joinson A. Causes and implications of disinhibited behavior on the Internet. In: Gackenbach J, ed. Psychology and the Internet: Intrapersonal, Interpersonal and Transpersonal Implications. San Diego: Academic Press; 1998:43–60
Joinson A. Social desirability, anonymity, and Internet-based questionnaires. Behav Res Methods Instrum Comput 1999;31:433–438
Kaldo V, Larsen HC, Andersson G. Internet-based cognitive-behavioral self-help treatment of tinnitus: a Clinical effectiveness and predictors of outcome. Am J Audio 2004;13:185–192
Kuppersmith RB. Is e-mail an effective medium for physician–patient interaction? Arch Otolaryngol Head Neck Surg 1999;125:468–470
Mair F, Whitten P. Systematic review of studies of patient satisfaction with telemedicine. BMJ 2000;320:1517–1520
Marrs RW. A meta-analysis of bibliotherapy studies. Am J Community Psychol 1995;23:843–870
Morin CM. Relief from Insomnia: Getting the Sleep of Your Dreams. New York: Doubleday; 1996
Norcross JC, Santrock JW, Campbell LF, Smith TP, Sommer R, Zuckerman EL. Authoritative guide to self-help resources in mental health. New York: Guilford Press; 2000
Reich GE. American Tinnitus Association and self-help groups. In: Tyler RS, ed. Tinnitus Handbook. San Diego: Singular/Thomson Learning; 2000:419–435
Scogin F, Floyd M, Jamison C, Ackerson J, Landreville P, Bissonnette L. Negative outcomes: What is the evidence on self-administered treatments? J Consult Clin Psychol 1996;64:1086–1089
Sheppard L, Hawkridge A. Tinnitus: Learning to Live with It. Bath, UK: Ashgrove Press; 1987
Ström L, Pettersson R, Andersson G. A controlled trial of self-help treatment of recurrent headache conducted via the Internet. J Consult Clin Psychol 2000;68:722–727
Tyler RS, ed. Tinnitus Handbook. San Diego: Singular/Thomson Learning; 2000
Vernon JA, ed. Tinnitus: Treatment and Relief. Boston: Allyn & Bacon; 1998
Wilson DM, Cash TF. Who reads self-help books? Development and validation of the self-help reading attitudes survey. Pers Individ Dif 2000;29:119–129
< div class='tao-gold-member'>



