Purpose
To develop a classification and grading system for myopic maculopathy.
Design
Development and evaluation of a classification system for myopic maculopathy based on observational case series.
Methods
A comprehensive set of myopic macular lesions was defined via literature review and through consensus meetings among retinal specialists and clinician scientists. A classification of myopic maculopathy was formulated based on fundus photographs and a modified Delphi process and consensus. Inter- and intraobserver reproducibility, assessed as agreement (%) and weighted kappa values, were evaluated. One hundred retinal photographs with myopia and myopic macular lesions were selected from case series at the High Myopia Clinic of the Tokyo Medical and Dental University, Tokyo, Japan.
Results
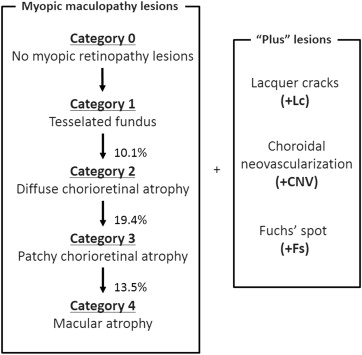
We defined 5 categories of myopic maculopathy including “no myopic retinal degenerative lesion” (Category 0), “tessellated fundus” (Category 1), “diffuse chorioretinal atrophy” (Category 2), “patchy chorioretinal atrophy” (Category 3), and “macular atrophy” (Category 4). Three additional features to supplement these categories were defined as “plus” lesions, namely, lacquer cracks, myopic choroidal neovascularization, and Fuchs spot. Posterior staphyloma was considered as a further, important sign of myopic retinopathy. The intraobserver agreement was ≥85% and the corresponding weighted kappa statistic was ≥0.6 between observations. After a brief training session, interobserver kappa statistics reached the predefined satisfactory level (≥0.4), considered as above moderate agreement.
Conclusions
We propose a classification system for myopic maculopathy that was found to be reproducible. Applying a uniform classification in different studies will facilitate communication and comparison of findings from clinical trials and epidemiologic studies.
Myopic maculopathy is one of the major causes of visual impairment and legal blindness worldwide, especially in East Asia. According to the Tajimi Study in Japan, myopic maculopathy is the third-leading cause of low vision and the leading cause of legal blindness. In the Shihpai Eye Study in Taiwan and the Beijing Eye Study, it was the second most frequent cause of visual impairment and blindness. Although myopia is less prevalent in Western countries, myopic maculopathy has also been reported to be a significant cause of legal blindness in the Western Hemisphere.
The principal alterations in pathologic myopia include excessive axial elongation of the globe and associated deformation of the posterior ocular segment, with posterior staphyloma an important primary sign. Secondary to the increased axial length and staphyloma formation, a range of retinal and choroidal lesions may develop in the posterior pole in eyes with pathologic myopia. These changes are termed myopic maculopathy. Curtin and Karlin proposed a definition of myopic maculopathy that included the features of chorioretinal atrophy, central pigment spot (“Fuchs spot”), lacquer cracks, posterior staphyloma, and optic disc changes.
After the initial definition of myopic maculopathy by Curtin and Karlin in 1970, the definition of myopic maculopathy has not been revised; thus there has been no commonly accepted classification of myopic maculopathy. Although several photographic grading schemes have been proposed in different epidemiologic studies ( Table 1 ), the definition of myopic maculopathy has not been consistent across studies. Owing to the lack of a common classification scheme, a direct comparison of the prevalence, incidence, and pattern of individual, typical myopic lesions has not been possible yet. Furthermore, with the introduction of anti–vascular endothelial growth factor (VEGF) for the treatment of myopic choroidal neovascularization (CNV), there is an urgent need for a standard photographic grading system with consistent nomenclature to classify the different phenotypes of myopic maculopathy, to be used by different studies to assess the utility of therapy. In epidemiologic study or clinic screening settings, angiography and optical coherence tomography (OCT) are not always available and therefore color retinal imaging is the primary tool with which initial diagnosis of myopic maculopathy is made.
| Study | Age (Years) | Race/Ethnicity | N | High Myopia | Any Myopic Macular Lesions | Posterior Staphyloma | Myopic Chorioretinal Atrophy | Lacquer Cracks | Fuchs Spot | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Definition | N | % | N | % Population (% High Myopia) | (%) | (%) | (%) | (%) | ||||
| Blue Mountains Eye Study, Australia | ≤49 | White | 3583 | ≤−5.0 D | 98 | 2.7 | 44 | 1.2 (44.9) | 26.5 a | 7.1 | 8.2 | 3.1 |
| Beijing Eye Study, China | ≤40 | Chinese | 4319 | <−5.0 D | 143 | 3.3 | 132 | 1.6 (92.6) | 48.4 a | 92.6 b | 5.6 | 2.1 |
| Handan Study, China | ≤30 | Chinese | 6603 | <−5.0 D | 139 | 2.1 | 60 | 0.9 (43.3) | 37.5 a | 25.2 | 18.8 | 7.2 |
| Hisayama Study, Japan | ≤40 | Japanese | 1892 | <−5.0 D | 108 | 5.7 | 33 | 1.7 (30.6) | – a | 29.7 d | 2.8 | – |
| Shihpai Study, Taiwan | ≤65 | Chinese | 1058 | <−6.0 D | 44 | 4.2 | 32 | 3.0 (72.2) e | – a | – c | – | – |
| Singapore Indian/Chinese Study | ≤40 | Chinese, Indian | 6680 | <−6.0 D | 332 | 5.0 | – f | 90.0 a | 23.0 c | 1.8 | 0 | |
a Classification by Curtin et al.
b Classification by Steidl and Pruett.
d Macular atrophy: 6.5%; patchy chorioretinal atrophy: 7.4%.
e Classification by Avila: M0: 6.8%, M1: 11.4%, M2: 9.0%, M3: 15.9, M4: 18.2%, M5: 38.6%.
f Classification by Avila: M0: 10.0%, M1: 58.4%, M2: 22.7%, M3: 0.9, M4: 5.5%, M5: 1.5%.
We therefore aimed to propose a classification system of myopic maculopathy to distinguish the severity of the disease, with a consensus among a number of retinal experts. We further assessed the intra- and interobserver agreement on myopic maculopathy lesion diagnosis following the classification system. By definition, peripheral retinal signs associated with high myopia were not covered in this classification system.
Methods
This study consisted of 2 phases: first, a consensus meeting to develop a classification system for myopic maculopathy; and second, assessment of the inter- and intraobserver agreement in applying the classification system to 100 selected fundus photographs of eyes with pathologic myopia, defined as having signs of myopic maculopathy in eyes with a myopic refractive error of greater than −8.0 diopters. This research adhered to the tenets of the Declaration of Helsinki, and the classification of myopic maculopathy and the retrospective review of patients records were approved by the Ethics Committee of Tokyo Medical and Dental University.
Consensus Meetings and Process to Formulate Classification System for Myopic Maculopathy
To formulate the classification system, discussions were held with experts in consensus meetings. An initial draft of a classification system was developed based on the study by Hayashi and associates with additional information obtained from a literature review, textbooks, and longitudinal observations of approximately 3500 patients with pathologic myopia collected at the High Myopia Clinic of the Tokyo Medical and Dental University, Tokyo, Japan. We defined the macula area as the region of the macula grid used in the International Classification and Grading System for Age-related Maculopathy and Age-related Macular Degeneration ( Supplemental Figure 1 , available at AJO.com ).
Assessment of Inter- and Intraobserver Agreement to Confirm Reproducibility of Proposed Classification System
Five observers were trained to use the classification system and then asked to apply the classifications to a set of 100 images, which all included at least 1 myopic maculopathy sign in eyes with high myopia (median age: 64.0 years, median axial length: 30.08 mm, interquartile range: 28.66-31.67 mm). Proportions of eyes with each lesion type are shown in Supplemental Table 1 (available at AJO.com ). A senior retinal specialist (K.O.M.), 2 retinal specialists (M.M., R.K.), an ophthalmology resident (K.S.), and a trained retinal image grader (Y.K.) graded the same 100 images twice without other clinical information. Intra- and interobserver agreement (% of cases agreed between 2 assessments by the same [intra-] and different [inter-] observers) and the weighted kappa statistics were calculated. Using the diagnosis made by the senior retinal specialist (K.O.M.) as a reference, intergrader agreement and weighted kappa statistics were calculated. The weighted kappa statistic (κ) was considered as “moderate” if κ ≥ 0.4, “good” if κ ≥ 0.6, and “excellent” if κ ≥ 0.8. If the weighted kappa statistic did not reach at least moderate agreement, group sessions were conducted to discuss challenging cases in order to improve the classification system, until moderate agreement was reached.
Results
Formulation of Proposed Classification for Myopic Maculopathy and Related Lesions
We first identified 3 papers proposing classification for myopic maculopathy in detail. The first paper was by Curtin and Karlin and proposed 5 fundus changes associated with increased axial length of the eye, namely, optic nerve crescent, chorioretinal atrophy, central pigment spot (Fuchs spot), lacquer cracks, and posterior staphyloma. This classification has a limitation in that it does not cover all the myopic maculopathy lesions (eg, CNV), nor does it provide detailed differentiation between diffuse and patchy chorioretinal atrophy. The second paper was by Avila and associates, proposing a scale of macular changes that integrated tessellation (M1), posterior staphyloma (M2), lacquer cracks (M3), focal choroidal atrophy (M4), and large geographic atrophy (M5). The third paper was by Hayashi and associates, who described detailed myopic maculopathy lesions and scheme of progression. Although we acknowledged that Avila’s classification has been widely used in previous studies ( Table 1 ), there are limitations in that some cases do not progress in the order of this proposed scale and there are cases that cannot be categorized in any of the categories (eg, eyes with lacquer cracks but without staphyloma cannot be categorized M2 or M3 in Avila’s classification). The paper by Hayashi and associates has proposed a detailed classification and covers all the myopic maculopathy lesions, together with a suggested pattern of progression based on longitudinal observation of 12.7 years. Therefore, in our proposed classification, we have adopted the scheme of progression described by Hayashi and associates to complement the classification systems proposed by Curtin and Karlin, Avila and associates, and other publications. Overall definitions of myopic maculopathy are shown in Table 2 (detailed definitions can be found in Table 3 and Supplemental Table 2 , available at AJO.com ).
| Myopic Maculopathy | “Plus” Lesions | ||
|---|---|---|---|
| Category 0 | No macular lesions | + | Lacquer cracks (Lc) Choroidal neovascularization (CNV) Fuchs spot (Fs) |
| Category 1 | Tessellated fundus | ||
| Category 2 | Diffuse chorioretinal atrophy | ||
| Category 3 | Patchy chorioretinal atrophy | ||
| Category 4 | Macular atrophy |
a Definitions of each lesion can be found in Table 3 and Supplemental Table 2 (available at AJO.com ).
| I. Myopic macular lesions |
| Tessellated fundus (Category 1) |
| Well-defined choroidal vessels that can be observed clearly around the fovea as well as around the arcade vessels ( Supplemental Figure 2 , available at AJO.com ) |
| Diffuse chorioretinal atrophy (Category 2) |
| Yellowish white appearance of posterior pole. When present, further estimate size and extent using disc area as a relative size unit. ( Supplemental Figure 3 , available at AJO.com ) |
| Patchy chorioretinal atrophy (Category 3) |
| Well-defined, grayish white lesions in the macular area or around the optic disc ( Supplemental Figure 4 , available at AJO.com ) |
| Macular atrophy (Category 4) |
| Well-defined, grayish white or whitish, round chorioretinal atrophic lesion in the foveal region; may appear around a regressed CNV (Fuchs spot) ( Supplemental Figure 5 , available at AJO.com ) |
| II. “Plus” lesions of the myopic macular lesions |
| Lacquer cracks |
| Yellowish linear lesions in the macula. Often criss-cross over the underlying choroidal vessels. Newly developed lacquer cracks may be seen with hemorrhage. ( Supplemental Figure 6 , available at AJO.com ) |
| Choroidal neovascularization |
| Lesion associated with CNV and exudation, hemorrhage, or serous retinal detachment at the posterior pole ( Supplemental Figure 7 , available at AJO.com ) |
| Fuchs spot |
| Pigmented grayish white scar of myopic CNV without associated exudation, and sometimes associated with pigmentation ( Supplemental Figure 8 , available at AJO.com ) |
| III. Posterior staphyloma ( Supplemental Figures 9 and 10 , available at AJO.com ) |
Local bulging of the sclera at the posterior pole of the eye, that has a radius of less than the surrounding curvature of the wall of the eye:
|
a Detailed definitions are shown in Supplemental Table 2 (available at AJO.com ).
b The inferior staphyloma involving the macula was not included in the original classification by Curtin.
Proposed Classification and Definitions of Myopic Maculopathy
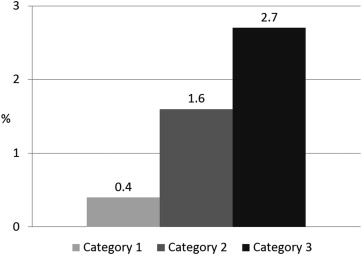
We categorized myopic maculopathy lesions into 5 categories of “no myopic retinal lesions” (Category 0), “tessellated fundus only” (Category 1), “diffuse chorioretinal atrophy” (Category 2), “patchy chorioretinal atrophy” (Category 3), and “macular atrophy” (Category 4) ( Figure 1 ). These categories were defined based on long-term clinical observation and the increasing risks of developing myopic CNV and macular atrophy associated with the increase in these categories from 1 to 3 ( Figure 2 ).
Proposed Definition of “Plus” Lesions Adding to the Category of Myopic Maculopathy
Three additional features leading to central vision loss were added to these categories and were included as “plus” signs. These features are: (1) lacquer cracks (Lc); (2) myopic CNV, and (3) Fuchs spot (Fs), ( Table 2 ). The reason for separately defining “plus” signs is that those 3 lesions (Lc, CNV, and Fs) do not fit into any particular category, and can develop from, or coexist, in eyes with any of the myopic maculopathy categories.
Proposed Definition of Posterior Staphyloma
Posterior staphyloma was defined based on Curtin’s classification. We recategorized and simplified Curtin’s classification according to the involvement of the macula, size, and location relative to the macula and the optic disc ( Table 3 ; Supplemental Table 2 , Supplemental Figures 9 and 10 , available at AJO.com ).
Inter- and Intraobserver Agreement Using Proposed Classification System
The average intraobserver agreement and the weighted kappa statistics of the 100 selected images graded by 5 independent observers are shown in Table 4 . The intraobserver agreement (%) for all graders when the same image was graded twice was ≥85% and the corresponding weighted kappa statistic was ≥0.6. The average interobserver agreement and weighted kappa statistic between the senior ophthalmologists and each of the graders are shown in Table 4 . At the initial assessment, weighted kappa statistics for tessellated fundus (2 graders), posterior staphyloma (1 grader), Fuchs spots (2 grader), and lacquer cracks (1 grader) did not reach the satisfactory level for weighted kappa statistics. Therefore, group discussion sessions were held to determine the reasons for the disagreements. We then reconfirmed the protocol details while referring to the standard (shown in Supplemental Figures 2-8 , available at AJO.com ) retinal images to clarify the relevant definitions. After a period of at least 1 month, all observers regraded the 100 images. The interobserver weighted kappa statistics in the second time grading reached the predefined satisfactory level of ≥0.4.
| Intraobserver Agreement | Interobserver Agreement a | ||||||
|---|---|---|---|---|---|---|---|
| Agreement % | κ | Standard Error | Agreement% | κ | Standard Error | ||
| Category 1 | Tessellated fundus | 96.1 | 0.69 | 0.09 | 94.5 | 0.56 | 0.08 |
| Category 2 | Diffuse atrophy | 88.3 | 0.72 | 0.09 | 87.7 | 0.59 | 0.10 |
| Category 3 | Patchy atrophy | 93.3 | 0.82 | 0.10 | 91.0 | 0.78 | 0.11 |
| Category 4 | Macular atrophy | 96.8 | 0.89 | 0.10 | 94.3 | 0.84 | 0.11 |
| “Plus” lesions | Lacquer cracks | 94.9 | 0.74 | 0.10 | 87.7 | 0.61 | 0.11 |
| Fuchs spot | 95.1 | 0.74 | 0.10 | 89.7 | 0.64 | 0.11 | |
| Posterior staphyloma | 85.1 | 0.63 | 0.09 | 79.8 | 0.52 | 0.09 | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


