International Perspectives
In our busy professional lives we rarely have an opportunity to consider how the work we do is being performed throughout the world. One might expect there to be significant differences and similarities in how we practice. How do the climate, the economy, government regulation and population demographics, customs and characteristics impact clinical practice in different countries? In a quest to gain a deeper understanding about refractive surgery as performed throughout the world this chapter will take the reader on a virtual voyage of exploration to China, Singapore, South Korea, Brazil, Germany, Turkey, and Israel. A set of questions was submitted to several of our international contributors. This survey included queries about the evolution of refractive surgery in the individual country, unique patient management pearls, equipment preferences, and business models. Through their responses it is hoped you will come to appreciate and gain insight from the similarities and differences in the practice of refractive surgery. We begin our virtual journey in Hong Kong.
CHINA (HONG KONG)
VISHAL JHANJI
Hong Kong has prospered under the “one country, two systems” policy since its handover to the Chinese government in 1997.1 An excellent infrastructure, including a sound banking system, a strong legal system, and ample foreign exchange reserves, enable Hong Kong to quickly respond to changing circumstances. With this dynamic background, ophthalmology here has managed to keep pace with the international advances.1 In fact, it is one of the top choices for medical graduates in Hong Kong.
Laser vision correction or refractive surgery is a very popular and commonly performed surgical procedure in Hong Kong. This may
be attributed to the high prevalence of myopia in the Chinese population2 as well as high life expectancy. Although nearly all the private as well as University-based ophthalmology clinics in the city provide refractive surgery services to about 7 million people in the city, this facility is not available in the public sector. Based in a private clinic affiliated to a University, we have an in-house refractive surgery suite for performing common refractive procedures such as LASIK and surface ablation. Although microkeratome-assisted LASIK was successfully being performed earlier, a femtosecond LASIK machine (iFS 150 kHz, AMO Inc.) was acquired about 2 years ago. There is a general trend toward performing more LASIK as compared to surface ablation or other refractive surgeries, without compromising on the safety of the patients. The major reason behind this choice is that the patients want to resume work as soon as possible after the surgery. We also encounter a considerable proportion of high myopia (>6 diopters [D]). These patients seek to be rid of spectacles and/or contact lenses in the quickest possible manner. Much like other countries, major reasons for denying surgery in Hong Kong are inadequate corneal thickness and suspicious corneal topography.3 We also have our own share of preoperative issues such as contact lens-induced dry eyes, lid margin disease, and retinal degenerations requiring prophylactic treatment before LASIK.
be attributed to the high prevalence of myopia in the Chinese population2 as well as high life expectancy. Although nearly all the private as well as University-based ophthalmology clinics in the city provide refractive surgery services to about 7 million people in the city, this facility is not available in the public sector. Based in a private clinic affiliated to a University, we have an in-house refractive surgery suite for performing common refractive procedures such as LASIK and surface ablation. Although microkeratome-assisted LASIK was successfully being performed earlier, a femtosecond LASIK machine (iFS 150 kHz, AMO Inc.) was acquired about 2 years ago. There is a general trend toward performing more LASIK as compared to surface ablation or other refractive surgeries, without compromising on the safety of the patients. The major reason behind this choice is that the patients want to resume work as soon as possible after the surgery. We also encounter a considerable proportion of high myopia (>6 diopters [D]). These patients seek to be rid of spectacles and/or contact lenses in the quickest possible manner. Much like other countries, major reasons for denying surgery in Hong Kong are inadequate corneal thickness and suspicious corneal topography.3 We also have our own share of preoperative issues such as contact lens-induced dry eyes, lid margin disease, and retinal degenerations requiring prophylactic treatment before LASIK.
Another important issue for refractive surgeons in Hong Kong is the peculiar anatomy of Chinese eyes. It has been shown that there are considerable differences in Chinese eyes compared to their Caucasian counterparts.4 We frequently come across patients who have very small palpebral apertures and a wide nasal bridge (Fig. 17.1). Since iFS femtosecond machine is available only with a “one-size” suction ring, it is challenging at times to insert the ring into the patient’s eye during flap creation. Having cancelled a few surgeries due to inability to fit the suction ring in these eyes, we now routinely measure the horizontal and vertical palpebral aperture in all the patients. These patients are informed preoperatively that the surgery might have to be aborted in case the suction ring cannot be inserted into the eye intraoperatively. These patients are offered microkeratome-assisted LASIK or surface ablation in such scenarios.
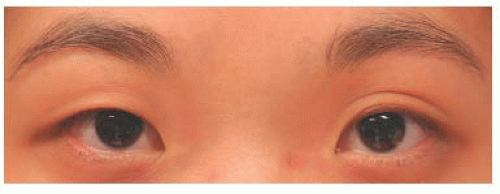 FIGURE 17.1 Chinese eyes often have small palpebral apertures with small corneal diameters. |
Another feature in ocular anatomy that is relevant to refractive surgery is small corneal diameter. In most of the cases, LASIK flap diameters are set at a lower value (typically 8.8 mm compared to 9.0 mm in Caucasian eyes). In many cases, the LASIK flap edge is close to the corneal limbus. Consequently, we encounter cases with intraoperative anterior chamber gas bubbles (Fig. 17.2). Likewise, we inform the patients about this potential complication during preoperative counseling.
Postoperative management and treatment protocol of refractive surgery patients match the international standards followed elsewhere. We do, however, encounter many steroid responders. This may be related to the degree of myopia as well as the prevalence of glaucoma in the Chinese5 people. These cases are detected well in advance and are managed appropriately.
 FIGURE 17.2 Bubbles (arrows) entered the anterior chamber during femtosecond laser flap creation in a patient with a small cornea. |
One more aspect that deserves mention is the popularity of femtosecond technology amongst the general population in Hong Kong. Since the time of acquiring femtosecond machine, the number of surgeries performed using a microkeratome at our center is <1%. This is in spite of the fact that all patients are offered both microkeratome as well as femtosecond surgery at the time of preoperative counseling. It is also interesting that although microkeratome LASIK is more economical compared to femtosecond LASIK everywhere in the city, nearly all patients prefer to receive femtosecond or “all laser surgery.” Upon inquiring the reason for choosing femtosecond over microkeratome, common responses include “peer pressure,” “new technology,” and “available online information.” It is only fair that people find femtosecond LASIK to be a more advanced and safer technology compared to other options. However, this behavior also reflects the paying capacity of an average patient in Hong Kong in the absence of any reimbursement by insurance agencies. To my knowledge, the cost of refractive surgery varies in Hong Kong from about US $1,500 to $4,000. Regardless, most of the refractive surgery centers are busy and flourishing. This further creates a lot of competition among different centers. It is not uncommon to see “discount slogans” all over the place offering concession on LASIK surgery.
Refractive surgery in Hong Kong is experiencing exciting developments parallel to the expansions in the field of laser vision correction surgeries. Most of the research is being conducted in University-based clinics, which continue to lure more patients by reducing the total cost of surgery. Yet I have come to believe that potential refractive surgery candidates in Hong Kong have confidence in receiving treatment in teaching hospitals such as ours, irrespective of the cost of the procedure. As mentioned earlier, longer life expectancy in Hong Kong is an additional blessing. We are treating more patients who are >50 years old and want to enjoy life free of spectacle or contact lenses. We hope to see refractive surgery becoming increasingly safer and accessible to all patients in Hong Kong.
Acknowledgments: I wish to thank all the doctors and staff in the University Eye Clinic of the Chinese University of Hong Kong, Hong Kong.
References
1. Lam DS, Tham CC. Ophthalmology in Hong Kong. Br J Ophthalmol. 2003;87(2):130-131.
2. Gao LQ, Liu W, Liang YB, et al. Prevalence and characteristics of myopic retinopathy in a rural Chinese adult population: the Handan Eye Study. Arch Ophthalmol. 2011;129(9):1199-1204.
3. Xu K, McKee HD, Jhanji V. Changing perspective of reasons for not performing laser-assisted in situ keratomileusis among candidates in a university eye clinic. Clin Exp Optom. 2013 Jan;96(1):20-24. doi:10.1111/j.1444-0938.2012.00730.x [Epub ahead of print].
4. Blake CR, Lai WW, Edward DP. Racial and ethnic differences in ocular anatomy. Int Ophthalmol Clin. 2003;43(4):9-25.
5. http://www.hkos.org.hk/public_18.shtml. Accessed January 1, 2012.
SOUTH KOREA
DONGHO LEE and HAKSUNG CHUNG
LASIK was first introduced to South Korea in the early 1990s. Since then, refractive surgery has been growing over the years in Korea. There are 3,600 ophthalmologists in Korea, and almost three-fourths of them are active in clinical practice. Three hundred thirty-six of them are actively performing refractive surgeries and are members of the Korean Society of Cataract and Refractive Surgery (KSCRS).
The prevalence of myopia in South Korea is very high, and is reported to be 54%.1 Most of the myopes in Korea have a strong desire for refractive surgeries, and many of them have already undergone refractive surgeries.
Based on a survey conducted by the KSCRS in 2007,2 LASIK was the most popular surgery among PRK, LASIK, and LASEK, although its popularity significantly decreased
from 78% in 1999 to 48% in 2007. LASEK, Epi-LASIK, and PRK were 36%, 10%, and 6%, respectively. In 2001, I (Dr. Lee) was the first in Korea to start using prophylactic intraoperative mitomycin-C during PRK, and reported a large case series of 1,000 patients with my colleagues.3 PRK with mitomycin-C has increased in popularity, and some Korean refractive surgeons prefer PRK with mitomycin-C to LASIK in their practice. For myopes with >8 D, phakic intraocular lens (IOL) implantation was preferred. Ever since the wavefront analyzer was introduced, the number of wavefront analyzer users has increased from 17% in 2002 to 65% in 2007 in Korea. When asked whether wavefront ablation improved vision, 62% of KSCRS members answered yes. Thirty percent of KSCRS members perform presbyopia surgery with multifocal laser procedure, and 70% of them are satisfied with the results. Multifocal corneal surgeries using excimer lasers were introduced in Korea in 2004, and now most of the laser companies provide presbyopia-correction programs. In my own study, presented at Korean and European ophthalmology meetings, multifocal corneal excimer laser surgery showed safe and effective correction of presbyopia for up to 90% of patients.
from 78% in 1999 to 48% in 2007. LASEK, Epi-LASIK, and PRK were 36%, 10%, and 6%, respectively. In 2001, I (Dr. Lee) was the first in Korea to start using prophylactic intraoperative mitomycin-C during PRK, and reported a large case series of 1,000 patients with my colleagues.3 PRK with mitomycin-C has increased in popularity, and some Korean refractive surgeons prefer PRK with mitomycin-C to LASIK in their practice. For myopes with >8 D, phakic intraocular lens (IOL) implantation was preferred. Ever since the wavefront analyzer was introduced, the number of wavefront analyzer users has increased from 17% in 2002 to 65% in 2007 in Korea. When asked whether wavefront ablation improved vision, 62% of KSCRS members answered yes. Thirty percent of KSCRS members perform presbyopia surgery with multifocal laser procedure, and 70% of them are satisfied with the results. Multifocal corneal surgeries using excimer lasers were introduced in Korea in 2004, and now most of the laser companies provide presbyopia-correction programs. In my own study, presented at Korean and European ophthalmology meetings, multifocal corneal excimer laser surgery showed safe and effective correction of presbyopia for up to 90% of patients.
VISX laser system was the most commonly used by KSCRS members (about 32%), followed by Technolas (20%) and Zeiss Meditec MEL-80 (17%). For LASIK flap creation, 34% of surgeons used Hansatome, 22% used Intra-Lase, and 18% used Moria M2 microkeratome. Femtosecond laser users are increasing, and 73% of doctors responded that it would further increase in the future.
Most of the refractive surgeons in Korea own their laser surgery system in their private clinics. Only a few laser surgery centers, if any, share a laser system with other surgeons. Thanks to less strict governmental regulation compared to FDA, Korean refractive surgeons are performing refractive surgery with new technologies, including multifocal laser surgery and a variety of phakic IOL implantation techniques.
References
1. Lee SJ, Kim JM, Yu BC, et al. Prevalence of myopia in 19-year-old men in Gyeongsangnam-do, Ulsan and Busan in 2002. J Korean Ophthalmol Soc. 2009;50(9): 1392-1403.
2. Shin KH, Shyn KH. 2007 survey for KSCRS members—current trends in refractive surgery in Korea. J Korean Ophthalmol Soc. 2009;50(10):1468-1474.
3. Lee DH, Chung HS, Jeon YC, et al. Photorefractive keratectomy with intraoperative mitomycin-C application. J Cataract Refract Surg. 2005;31(12):2293-2298.
SINGAPORE
WEE-JIN HENG
High myopia is very common in Asia, and one of the problems is insufficient corneal thickness for LASIK. Postoperative glare and haloes may be more apparent and prolonged due to higher power treatments or the need to shrink the treatment zone. In Singapore, air force pilots and navy divers are allowed to undergo PRK, but are not permitted to have LASIK.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


