Purpose
To compare interferon (IFN) beta with methotrexate (MTX) in the treatment of intermediate uveitis with macular edema.
Design
Monocentric, prospective, randomized, controlled clinical trial.
Methods
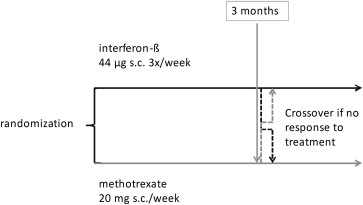
setting : Specialized uveitis center at the University of Heidelberg. patient or study population : Patients with either primary intermediate uveitis or uveitis associated with multiple sclerosis. main inclusion criteria : Visual acuity of 20/30 or worse (0.2 logarithm of the minimal angle of resolution) and macular edema of more than 250 μm (central 1-mm in optical coherence tomography; Stratus). Randomization into either IFN beta 44 μg subcutaneously 3 times weekly or 20 mg MTX subcutaneously once weekly. main outcome measures : At 3 months, the primary outcome parameter of mean change in visual acuity was evaluated and efficacy was determined. Secondary parameters were macular edema by optical coherence tomography, inflammatory activity, and retinal sensitivity by microperimetry (MP-1; Nidek). In case of treatment failure, switching to the other treatment arm was possible.
Results
Nineteen patients were included. Ten were randomized to MTX, and 9 were randomized to IFN beta. At 3 months, visual acuity improved a mean 0.31 logarithm of the minimal angle of resolution (range, −0.02 to −0.96, 15.6 letters on the Early Treatment Diabetic Retinopathy Study chart) in the IFN beta group versus a mean 0.09 logarithm of the minimal angle of resolution (range, 0.12 to −0.38, 4.7 letters) in the MTX arm ( P = .0435, Mann–Whitney U test). Macular thickness decreased by a mean of 206 μm (range, −41 to −416 μm) in the IFN arm, but increased by 47 μm (range, 108 to −28 μm) in the MTX group ( P < .0001).
Conclusions
Although the sample size is small, results of the trial support superiority of IFN beta over MTX in the treatment of macular edema in the setting of intermediate uveitis
Intermediate uveitis is characterized by cellular infiltration of the vitreous. Approximately 25% of patients with uveitis have intermediate uveitis and approximately 10% of them have comorbid multiple sclerosis. Intermediate uveitis therefore is, apart from optic neuritis, the typical manifestation of multiple sclerosis in the eye. Intermediate uveitis often is accompanied by macular edema, which is one of the main reasons for vision loss and which does not respond well to immunosuppressive therapy.
In a pilot study, we tested interferon (IFN) beta in multiple sclerosis-associated intermediate uveitis. Retrospectively, 13 patients were included, and in 82%, macular edema resolved. Thirteen patients (8 female, 5 male) with proven multiple sclerosis and associated uveitis in 25 eyes from 5 uveitis centers were treated with IFN beta-1a. Visual acuity (VA) improved in 17 eyes (71%), 5 eyes did not change (21%), and 2 eyes deteriorated (8%) because of development of cataract. Cystoid macular edema resolved after or during IFN beta treatment in 82% of the eyes. Although interferons are an accepted treatment for multiple sclerosis, it is not an approved treatment for uveitis. Several case series have shown efficacy for interferon alfa for ocular Behçet disease and other uveitis entities. Deuter and associates published a retrospective case series of 24 patients and reported the effect of interferon alfa on macular edema. So far, no randomized clinical trial for any of the IFNs has been published. We aimed to test the efficacy and safety of IFN beta in a prospective, randomized clinical trial comparing to methotrexate (MTX) as standard immunosuppressive therapy in patients with intermediate uveitis and inflammatory macular edema.
Methods
Local institutional review boards (Ethikkommission der medizinischen Fakultät Heidelberg, Heidelberg, Germany) and federal authorities (Bundesinstitut für Arzneimittel und Medizinprodukte, Bonn, Germany) approved the full protocol; patient information as well as written informed consent was obtained as required by German law (Arzneimittelgesetz) before study initiation (EudraCT number, 2004-004403-37). The clinical trial was registered at www.clinicaltrials.gov ( NCT00344253 ). The research described adhered to the tenets of the Declaration of Helsinki, and Health Insurance Portability and Accountability Act rules were observed. This prospective, randomized, controlled clinical trial was performed at a specialized uveitis center at the University of Heidelberg. Regular monitoring of data by an external monitor took place. Randomization, biostatistical calculations, and evaluations were carried out in cooperation with a biostatistician (Koordinationszentrum Klinische Studien, Heidelberg, Germany).
Patients 18 years or older with intermediate uveitis of at least 1 year’s duration with inflammatory macula edema either with or without associated multiple sclerosis could be included. Multiple sclerosis was diagnosed or excluded by magnetic resonance imaging, spinal fluid analysis, and neurologic examination performed by one of the authors (B.S.-H.). Other uveitis entities such as infectious or other autoimmune diseases, for example, sarcoidosis-associated uveitis, were excluded by history, physical examination, and chest radiograph as well as usual laboratory examinations. There had to be macular edema present with central 1-mm measures of 250 mm or more (determined using Stratus OCT; Zeiss, Jena, Germany) and 20/30 or worse VA (0.2 logarithm of the minimal angle of resolution [logMAR]). All patients included in the study had to have insufficient response to oral prednisone (at least 0.5 mg/kg body weight over a period of 4 weeks) and acetazolamide. All patients also had to have received local injections in the past (at least 3 months before study entry). Main exclusion criteria were a diagnosis of depression or a history of suicide attempts, ocular triamcinolone injection within 3 months, current oral prednisone of more than 10 mg/day, or other associated diseases or infectious uveitis (for a complete list, see http://clinicaltrials.gov/ct2/show/NCT00344253?term=team+uveitis&rank=1 ).
The primary outcome criterion was mean change in best-corrected BCVA on Early Treatment Diabetic Retinopathy (EDTRS) charts at 3 months as compared with baseline. Standardized refraction was performed at each visit. A change of more than 2 lines (ie, 11 letters or more on Early Treatment Diabetic Retinopathy charts) was deemed significant. Secondary outcome criteria were improvement of macular edema (determined using Stratus OCT), intraocular inflammatory activity (anterior chamber cells and vitreous haze ), rate of ocular complications (eg, neovascularization and change in retinal sensitivity, assessed using 10-degree visual field testing with fundus perimetry [MP1, Nidek Technologies, Padova, Italy]). An increase of 2 dB was deemed significant. Quality of life was measured by 25-item National Eye Institute Visual Function Questionnaire (NEI VFQ-25) and the 36-item Short-Form Health Survey. Questions about adverse events (AEs) were posed systematically, and answers were documented at each visit. Safety laboratory examinations took place at each visit. Patients were randomized to treatment with either IFN beta (Rebif; Merck-Serono) 22 μg subcutaneously 3 times weekly for 2 weeks, then 44 μg 3 weekly, or MTX 20 mg subcutaneously once weekly.
Assuming a standard deviation of VA change of 2 lines, a relevant difference of 2 lines in comparison with baseline will show a difference between groups with 80% power and a significance of α = 0.05 when 17 patients are included in each group. On this basis of a difference of 2 lines in ETDRS visual acuity, a study sample of 34 patients was planned initially. Because during the trial the difference in VA gain between the groups was higher than expected, the protocol was recalculated in cooperation with a biostatistician, and a lower number of cases of at least 17 patients total was fixed by an amendment to the protocol.
One study eye was defined as the worse eye fulfilling inclusion and exclusion criteria. If both eyes were affected equally, the primary investigators (M.D.B. and F.M.) decided on the eye. After 3 months, outcome parameters were assessed. In case of treatment failure at the 3-month time point, switching to the other treatment arm was possible (for study design, see also Figure 1 ; numbers that crossed over can be seen in Figure 2 , the Consolidated Standards of Reporting Trials [CONSORT] diagram). The last study visit was at 1 year after screening.

Statistical Analysis
A linear regression model with baseline and 3 months’ difference was used. For the descriptive data analysis, means and ranges were calculated. Comparing the medians of groups of other possible risk factors, the Wilcoxon test, Fisher exact test, and Mann–Whitney U test were used where appropriate. Prism version 4.02 (GraphPad, San Diego, California, USA) was used for data analysis. For the modeling of the number of lines identified completely and the logMAR value, the last observation carried forward method was used, meaning that in case a subject did not come to the 3-month visit, VA values of the last visit nearest to the 3-month visit were used. A significance level of P = .05 was chosen to reject the null hypothesis.
Results
Demographic Details
Because of the strong superiority of the IFN-treated group, the study was terminated prematurely for ethical reasons. Instead of the planned 34 participants, 19 patients were included in the trial. Nine were randomized to receive IFN beta and 10 were randomized to receive MTX (see Figure 2 , CONSORT diagram). Groups were comparable regarding gender, age, VA, and OCT measurements at baseline, but differed slightly because more patients with multiple sclerosis were included in the MTX arm (n = 4) than in the IFN beta arm (n = 1; see Table 1 ). Inflammatory activity was low in both groups at baseline, with means of 0.56 and 0.45 vitreous haze, respectively (range, 0 to 1).
| IFN | MTX | P Value a | |
|---|---|---|---|
| Median age (y) | 41 | 42 | .7802 |
| Multiple sclerosis (%) | 11 | 40 b | |
| Female (%) | 78 | 60 | |
| Mean vitreous haze | 0.56 | 0.45 | .7802 |
| Mean logMAR VA (Snellen equivalent) | 0.48 (20/60) | 0.34 (20/40) | .2775 |
| Mean OCT at baseline (μm) | 430 | 371 | .2775 |
Primary Outcome Visual Acuity
At 3 months, patients in the IFN beta arm showed a mean improvement in VA of 0.31 logMAR (range −0.02 to −0.96 logMAR; 15.6 letters on Early Treatment Diabetic Retinopathy charts; P = .0039, Wilcoxon signed-rank test) versus 0.09 logMAR (range, 0.12 to −0.38 logMAR; 4.7 letters on Early Treatment Diabetic Retinopathy charts) in the MTX arm ( P = .1309; see Table 2 and Figure 3 ). Comparing the VA change between groups showed a significant difference ( P = .0435, Mann–Whitney U test). Looking at proportions, 5 patients (56%) in the IFN group versus 3 patients (38%) in the MTX group improved by more than 2 lines, which was not statistically significant ( P = .3992, Fisher exact test). Interestingly, from the 4 patients with multiple sclerosis randomized into the MTX group, 2 responded with regard to VA.
| IFN | MTX | P Value a | |
|---|---|---|---|
| Mean vitreous haze at 3 months | 0.16 | 0.44 | .1903 |
| Mean logMAR VA (Snellen equivalent) | 0.16 (20/30) | 0.25 (20/40) | .0435 |
| Mean OCT (μm) | 228 | 409 | <.0001 |
a Mann–Whitney U test for the difference between baseline and 3-month measurement.
Secondary Outcome Criteria
At 3 months, 9 patients (100%) in the IFN beta group but only 2 patients (25%) in the MTX group showed improvement in macular thickness ( P = .0023, Fisher exact test) with a mean decrease in thickness of 206 μm (range, −41 to −416 μm; P = .0039, Wilcoxon signed-rank test) versus a mean increase of 47 μm (range, 108 to −28 μm; P = .0781; Table 2 and Figure 4 ). The difference in OCT thickness measurement at 3 months as compared with baseline was statistically significant between groups ( P < .0001, Mann–Whitney U test). This was mirrored by a mean increase of 2.9 dB (range, −1.6 to 7.2 dB) in foveal MP-1 measurements in the IFN beta group and 0.3 dB (range, −3.8 to 3.6 dB) in the MTX arm ( P = .0464, Mann–Whitney U test).
Looking at the evolution of macular edema as judged by the investigator, there were only 2 patients with macular edema left in the IFN beta group versus 7 in the MTX arm ( P = .015, Fisher exact test). Inflammatory activity improved in the IFN beta arm to a mean 0.16 vitreous haze (median haze, 0; range, 0 to 0.5) and remained unchanged with a mean 0.44 (median, 0.5; range, 0 to 1) in the MTX arm ( P = .1903, Mann–Whitney U test). Anterior chamber cell count remained unchanged at 0 to trace cells.
Study Evaluation After the 3-Month Time Point
All nine (100%) patients in the IFN beta group remained in the study and received IFN beta. Six MTX patients (75%) decided to switch treatment arms, as permitted in the protocol. The remaining 2 patients did not wish to stay in the study (see Figure 2 , CONSORT diagram). After switching treatments, VA improved in these patients, with a mean increase of 0.32 logMAR (range, 0.13 to 0.48 logMAR) at the 1-year study end (see Figure 3 , Bottom). VA remained stable or improved further in those patients who continued to receive IFN beta (mean, 0.36-logMAR VA increase at 1 year as compared with baseline; range, 0.06 to 0.94 logMAR).
OCT improved in the former MTX arm after switching to IFN beta by a mean 191 μm (range, 37 to 382 μm) at the 1-year study end and in the original IFN beta arm by a mean of 289 μm (range, 29 to 426 μm) as compared with baseline (see Figure 4 ).
Fundus perimetry improved further in both groups, with a mean increase of 5.0 dB foveal sensitivity in the patients treated directly with IFN beta. Fundus perimetry improved by 3.4 dB in the patients who switched to IFN beta after the 3-month time point. Clinically at the 1-year time point, macular edema was still seen in 1 patient in the IFN beta arm and in 3 patients in the MTX arm after switching.
Inflammatory activity improved further as well. At 1 year, no sheathing was seen, vitreous haze was down to 0 in 9 patients in the IFN beta arm and in 5 patients formerly in the MTX arm after switching to IFN beta; the remaining patient showed 0.5+ haze.
Adverse Events
One serious AE was reported in the trial, which was judged to be unrelated to the study treatment (hypertensive crisis in a patient receiving IFN beta that required hospitalization in a patient previously known to have arterial hypertension). A total of 48 AEs was reported in the IFN beta arm versus 27 AEs in the MTX arm. The mean number of AEs in the IFN beta arm was higher, with a mean of 5.3 per patient (range, 1 to 11) versus 2.7 in the MTX arm (range, 0 to 9; P = .0279, Mann–Whitney U test). The most frequent AEs are shown in Table 3 . Flu-like symptoms, known to be frequent in IFN beta treatment, made up nearly half of the AEs in the IFN beta arm. All but 1 patient reported flu-like symptoms at least once, but they were mild in intensity and tolerable with concurrent paracetamol or ibuprofen use. The most frequent AE in the MTX arm was nausea, also a well-known side effect of that treatment. Infections were reported more frequently in the MTX arm, but were all mild short-term infections, such as pharyngitis or urinary tract infections. Depression or even suicidal thoughts were inquired about, but did not occur in our patient cohort.



