Instrumentation and Surgical Adjunctive Techniques for Macular Surgery
Masahito Ohji
Yasuo Tano*
*Deceased
INTRODUCTION
Instrumentation and techniques, key elements in vitreous surgery, have been developed and modified over the years. As a result of improvements in instrumentation and techniques, better results are being achieved and indications for vitreous surgery have expanded. Moreover, there have been numerous developments in instrumentation and adjunctive techniques since the publication of the first edition of “Macular Surgery” in 2000. For example, the 25-gauge or 23-gauge transconjunctival sutureless vitrectomy systems combined with a bright illumination system with a xenon light source are the biggest breakthroughs in vitreous surgery in the last decade. Adjunctives have also been developed, including various dyes for staining the internal limiting membrane (ILM) and antivascular endothelial growth factor (VEGF) medications. In this chapter, we describe new instrumentations and adjunctive techniques.
INSTRUMENTATION
Sutureless Transconjunctival Vitrectomy
The small 25-gauge and 23-gauge transconjunctival vitreous surgery systems are among the biggest innovations in the history of vitreous surgery. The specific features of small-gauge vitreous surgery include small instruments, the transconjunctival trocar system, and the absence of suture placement at the end of the vitreous surgery.
25-Gauge Vitrectomy System
Various kinds of instruments have been developed since Fujii et al. (1) introduced 25-gauge vitrectomy. Trocars, light pipes, and the vitreous cutter are the essential instruments in every surgery. Other instruments including the diathermy probe, laser probes, extendable curved pick, aspirating pick, various forceps, vertical scissors, curved scissors, and silicone-tipped brush back-flush needles have become available (2).
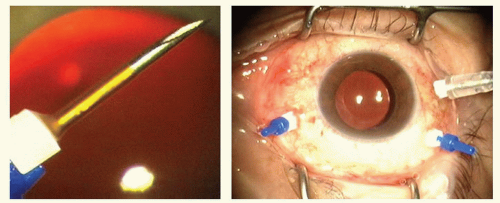 Figure 16-1. Trocars. |
Trocars
Trocars (Fig. 16-1) are essential for the 25-gauge sutureless transconjunctival vitrectomy system; some surgeons have used trocars even in the 20-gauge system. It is difficult to insert and remove instruments through both the conjunctiva and the sclera without the trocar system. Trocars also minimize damage to the wound, which is essential to prevent fluid leakage from the wound at the end of surgery.
Vitreous Cutters
There are two different kinds of vitreous cutters (Fig. 16-2). One is the pneumatic cutter driven by air pressure and the other is motor driven. Each has advantages and disadvantages. The pneumatic cutter is light and has minimum vibrations, while the motor-driven cutter allows more precise control of the blade motions. The performance of the pneumatic vitreous cutter has been improved, and the maximum cutting speed reaches as high as 2,500 per minute as in the 20-gauge system. A new generation of vitreous machines will be available soon with a vitreous cutter with a maximum cutting speed of 5,000 per minute. Because of the narrow aperture of the vitreous cutter, the aspiration rate is smaller than that of the 20-gauge cutter. Therefore, the aspiration vacuum is usually set to 500 to 600 mm Hg instead of 200 mm Hg to achieve sufficient aspirating flow (1).
23-Gauge Vitrectomy System
Eckardt (3) developed the 23-gauge vitrectomy system (Fig. 16-3), which has several similarities to the 25-gauge system and some differences. The 23-gauge steel trocars can be reused; disposable trocars are also available. The trocars in the 23-gauge system are inserted obliquely following the use of the MVR blade, while a one-step insertion system is also available (Fig. 16-4). In each system, an oblique wound pathway is
essential to prevent fluid leakage, because the scleral and conjunctival wound is obviously larger in the 23-gauge than in the 25-gauge system. The infusion rate and the aspiration rate are higher in the 23-gauge system than in the 25-gauge system. There is a considerable amount of balanced saline solution (BSS)/air flow through the trocars when the instruments are removed. Therefore, a plug or a valve attached to the trocars should be frequently used to prevent large consumption of BSS that might increase inflammation and prevent retinal damage by vigorous air flow (Fig. 16-5). The shafts of the 23-gauge instruments are much stiffer and can be used just like the 20-gauge instruments.
essential to prevent fluid leakage, because the scleral and conjunctival wound is obviously larger in the 23-gauge than in the 25-gauge system. The infusion rate and the aspiration rate are higher in the 23-gauge system than in the 25-gauge system. There is a considerable amount of balanced saline solution (BSS)/air flow through the trocars when the instruments are removed. Therefore, a plug or a valve attached to the trocars should be frequently used to prevent large consumption of BSS that might increase inflammation and prevent retinal damage by vigorous air flow (Fig. 16-5). The shafts of the 23-gauge instruments are much stiffer and can be used just like the 20-gauge instruments.
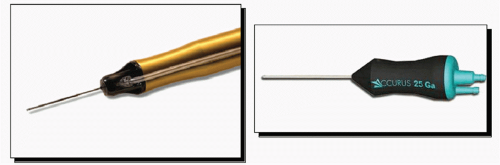 Figure 16-2. A 25-gauge vitreous cutter driven by motor (left) and 25-gauge vitreous cutter driven by air pressure (right). |
 Figure 16-3. A 23-gauge trocar-cannula system and pressure plate. |
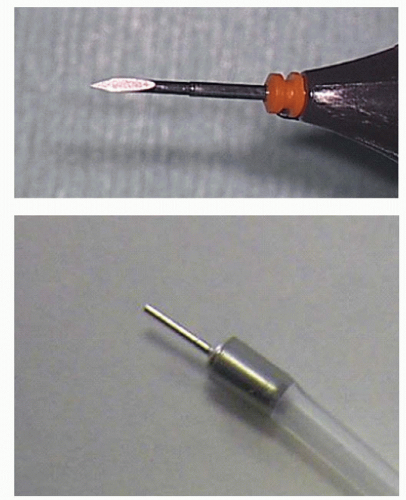 Figure 16-4. A 23-gauge disposable one-step trocar-cannula. The irrigation cannula (below) inserts easily through the trocar (above). |
Other 25- or 23-gauge Instruments
Many other instruments including the diathermy probe, laser probes with and without illumination, extendable curved pick, aspirating pick, various forceps, vertical scissors, curved scissors, and silicone-tipped brush back-flush needles have become
available (Figs. 16-6 and 16-7) (2). These instruments expand the indications for the 25-gauge sutureless vitrectomy.
available (Figs. 16-6 and 16-7) (2). These instruments expand the indications for the 25-gauge sutureless vitrectomy.
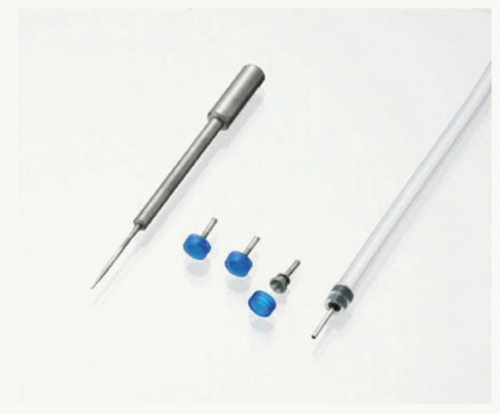 Figure 16-5. Closure valve for 23-gauge cannula to prevent leakage. |
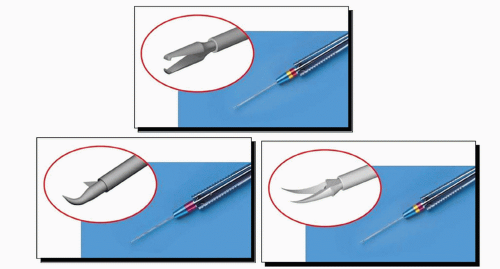 Figure 16-6. Forceps, vertical scissors, and curved scissors. |
The pressure plate developed by Eckardt (3) displaces the conjunctiva and allows the trocars to be inserted into the appropriate position (Fig. 16-3). A pressure plate was developed for the 23-gauge system; however, it is also useful with the 25-gauge system. The forceps have two scale marks on the top surface and on the serrated undersurface of the tip, and can be used in a similar fashion (Fig. 16-8) (4). The distance between the two scale marks is 4 mm. The scale marks can be used for accurate measurement and the serrated undersurface is useful to pull the conjunctiva.
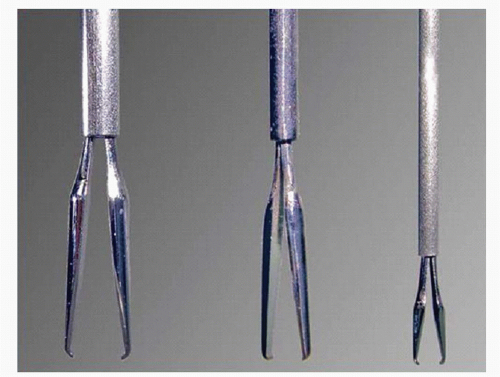 Figure 16-7. Comparison of 20-gauge (left), 23-gauge (center), and 25-gauge forceps (right). |
Bright Light Source
Endoillumination is one of the most important instruments used during vitreous surgery, and very bright endoillumination without light toxicity is extremely important. The light pipe in the 25-gauge vitrectomy system is narrower than that in the 20-gauge vitrectomy system, and the 25-gauge light pipe connected to the regular illumination source offers dim illumination and does not allow visualization of the details of the fundus lesions. A bright illumination system using a xenon light source or mercury vapor light source has been developed (Fig. 16-9).
The xenon light source combined with a good reflector can provide much brighter light than a regular halogen light source. The xenon light system provides very bright illumination even through a narrow 25-gauge light pipe that facilitates visualization of the details of the fundus lesions. A xenon light source can provide brighter light than the regular halogen light source; however, the xenon light provided contains more blue components than the halogen light. Surgical fields illuminated by the xenon light appear whiter or pale compared to the halogen light. In addition, the light toxicity associated with the blue component of the light is a consideration. Light wavelengths shorter than 550 nm are hazardous to the retina; therefore, the blue components of a wavelength shorter than 550 nm have to be filtered. By filtering the blue components of a wavelength shorter than 550 nm, the retinal safety is dramatically improved by approximately eight times (Table 16-1).
A xenon light source allows sufficient illumination through the narrow 25-gauge light pipe; however, the flexibility of the 25-gauge light pipe is still problematic. A shorter light pipe was
designed as a solution (5) (Fig. 16-10). Sufficient illumination can be provided through the shorter 25-gauge light pipe and it would be safer than the regular light pipe with respect to light toxicity and mechanical damage.
designed as a solution (5) (Fig. 16-10). Sufficient illumination can be provided through the shorter 25-gauge light pipe and it would be safer than the regular light pipe with respect to light toxicity and mechanical damage.
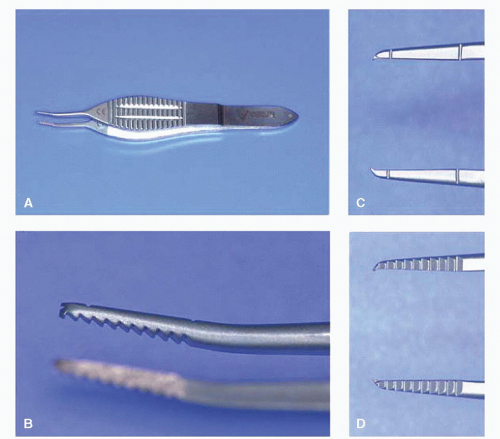 Figure 16-8. Forceps with scale marks. |
Mercury vapor is another light source alternative to provide brighter illumination than xenon light (Fig. 16-9). Brighter illumination is superior during surgery; however, light toxicity is also an important consideration. It has a filter system that reduces light toxicity and provides green light.
The 25-gauge vitrectomy system might not have been widely accepted without the bright illumination, because vitrectomy under dim illumination through a narrow 25-gauge light pipe with a halogen light source is not efficient or safe. The improvement in illumination made the 25- and 23-gauge vitrectomy systems easier, more efficient, safer, and expanded the indications for small-gauge vitrectomy.
The chandelier system has been available for a long time; however, its usefulness was limited because of insufficient illumination. The 25-gauge chandelier illumination system is another instrument that became useful after the introduction of the bright xenon light source (Fig. 16-11). The system allows surgeons to remove peripheral vitreous or to apply laser to the peripheral retina with scleral indentation by themselves when the chandelier is inserted into the trocar in the 25-gauge system. Recently, a 27-gauge chandelier system with a 29-gauge light fiber became available, which provides sufficient illumination without fluid leakage from the scleral wound at the end of surgery (6) (Fig. 16-11). The illuminated cannula also becomes useful when connected to the xenon light source or mercury vapor light source, although the illuminated cannula without a bright light source with dim illumination is available (Fig. 16-12).
In addition to its usefulness with the small-gauge vitrectomy system, the new light source is also useful in the 20-gauge system. The chandelier illumination, used as the fourth port, allows surgeons to perform bimanual techniques with standard 20-gauge instruments. The bimanual technique is useful and almost essential for treating complicated cases including severe proliferative diabetic retinopathy (PDR) or severe proliferative vitreoretinopathy (PVR); however, the bimanual technique required additional instruments including illuminated forceps and illuminated scissors. The 25/27-gauge chandelier illumination system allows surgeons to use hundreds of standard 20-gauge instruments including forceps, scissors, diathermy, aspiration needle, and laser probes.
Wide-Angle Viewing System
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


