4 Instrumentarium
During recent decades, with the growing popularity of endoscopic sinus surgery, a great variety of useful instrumentshave been designed. Special sets are offered by different companies, labeled with the names of renowned rhinosurgeons. It is not easy for the beginner to decide on one of these recommended sets or to put together their own set selected from different producers. Experienced rhinosurgeons do well with a combination of few instruments, but the particular design and the quality of the instruments contributes considerably to the success of the surgical craft.
Auxiliary equipment, such as microdebriders, curved drills, lasers, computer-aided navigation, and even robotic equipment, was recently developed (reviewed by Kennedy 2006). These technical innovations will be briefly mentioned on the following pages, but have not yet found their definite evaluation for everyday practice.
Surgical Endoscope
Intracavity surgery demands a well-illuminated, sharp, and, at times, magnifi edfield of vision with no blindspots. The operating microscope is very useful when used through a wide portal in the upper part of the oral vestibule, and for transnasal surgery of the posterior ethmoid and sphenoid cavities, but it is unsuitable as soon as the surgeon wishes to see around corners into niches, recesses, or ducts. Angled telescopes are therefore indispensable, especially for intranasal surgery of the anterior ethmoids and the sphenoid cavity, particularly with access via the middle nasal meatus.
Rigid tubes with high luminous intensity and Lumina eyepieces (Wolf) or Hopkins rods (Storz) are preferred, with 25° (quasi straight), 70°, and 110° directions of view (Fig. 4.1). They are almost all wide angled.
Cold-light illumination is always used, provided by a powerful light source and conducted by a glass fiber bundle. In this way, illumination strengths up to 15000 lux (standard light source) are achieved. The viewing angle runs from -40° to + 120°, and the depth of focus extends from 10 to 80 mm. The surgeon must first accustom himself to the rapidly changing magnification of the target. For example, reducing the working distance from 30 to 10mm produces a magnification of 1.5-fold (Fig. 4.2a, b).
Flexible endoscopes provide poorer illumination and the image is less sharp. They are seldom used for surgery but are preferred for diagnostic endoscopy of the nasal ducts and the nasopharynx and can also be used for follow-up after antral or sphenoid sinusotomy (Fig. 4.3a, b).
Transendoscopic dissection is too inflexible, and paraendoscopic instrumentation has been developed instead. The instruments have a relatively narrow shaft, they can be introduced under optical control, and they can be moved freely (see Chapter 6).
The versatility of paranasal sinus endoscopes has been considerably extended by the incorporation of a suctionirrigation handpiece with interchangeable aspiration and irrigation on the end of the endoscope (Fig. 4.4). Freeing the lens of blood, secretions, and misting by irrigation keeps the field of vision clear, whereas the usual telescopes must be continually removed from the nose to allow them to be cleaned and demisted. Effective irrigation with a powerful jet of water is another requisite for undisturbed visualization of the surgical field. Integration into the handpiece has not yet been realized. The author utilizes the prototype of a separate curved suction tube with intermittent overpressure jet irrigation.
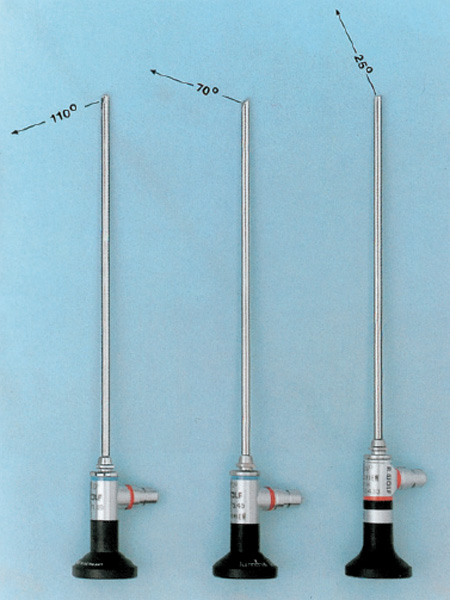
Fig. 4.1 Angled suction-irrigation telescopes for endoscopic sinus surgery. The most usual viewing angles are 25°, 70°, and 110°. High-illumination wide-angle objectives are usually preferred.
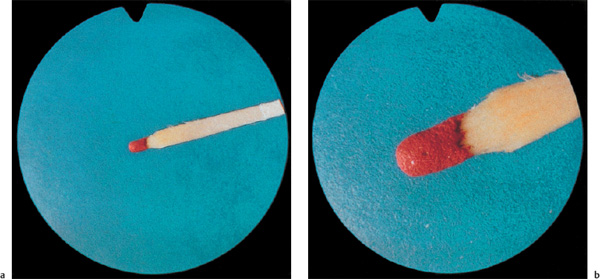
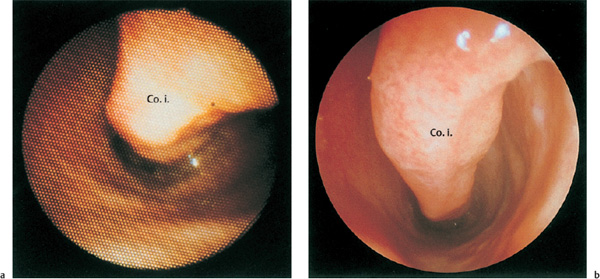
Fig. 4.3 a, b View of the left inferior meatus. a With a flexible endoscope. b With a 25° rigid telescope.
Other types of rigid endoscopes for ESS are on the market.
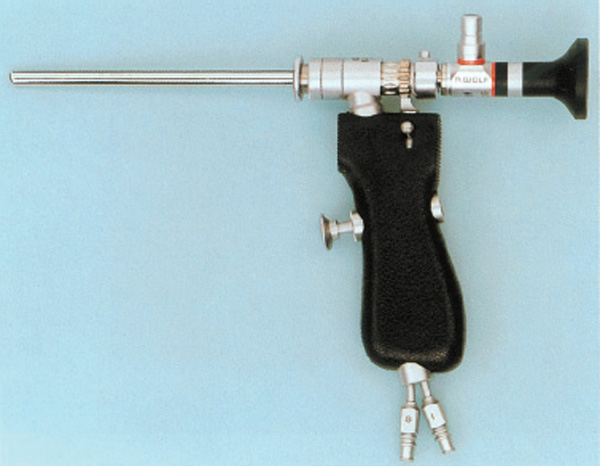
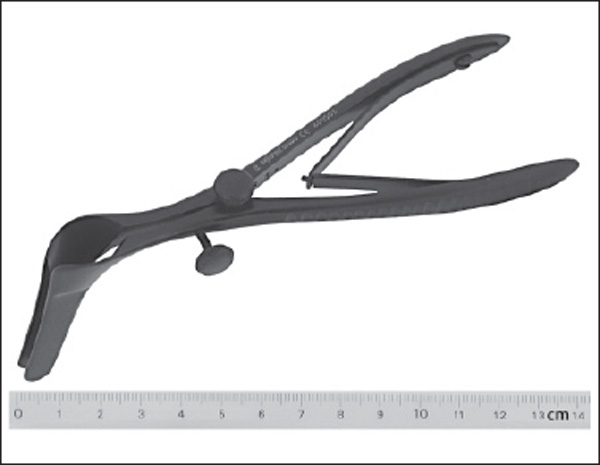
Fig. 4.5 Self-retaining nasal speculum for endonasal microscopy (cm scale).
The Microscope
Because every ENT specialist interested in endoscopic sinus surgery has been trained in otosurgery, the integration of a customary binocular microscope into the armamentarium of ESS need not be described in detail.
Its utilization offers some advantages in comparison with the telescope:
1. A free second hand can permanently clean the visual field with suction and irrigation.
2. The stereoscopic visualization of the target objects with adaptable magnification allows ideal microsurgical handling of dissectors and the CO2 laser.
These are reasons to make use of the microscope whenever its application is feasible. The opportunities, however, are drastically restricted by its limitation to direct, straightforward inspection of not-too-remote areas, whereas a telescope can easily be advanced even behind visual obstacles. For exposure of the most intranasal targets, a self-retaining speculum with long blades is a prerequisite (Fig. 4.5).
Combined telescopic and microscopic dissection can be beneficial, and is usually employed by the author for minute removal of tumors and malformations, especially at the sphenoid and posterior segments of the anterior skull base, and for all combined neurorhinosurgical interventions. The management of chronic hyperplastic or polypous sinusitis and of small and middle-sized dural defects, however, is predominantly in the realm of endoscopic sinus surgery.
Instruments
A wide range of instruments is available for transnasal surgery including fine, slender scalpels, fissure knives, perforators, rasps, and punches with varying angles of jaws and shaft.
Punches and forceps with various curves of the handle are suitable for resection of bony walls. New sharp cutting punches are still being developed to allow removal of tissue with preservation of neighboring mucosa. The diamond burr and sharp curettes should be used for removing bone, e. g., to widen a narrow frontal duct.
Equipment for the handling of tissues can be divided into tools for their visualization and severance, those for dissection, and those for hemostasis (Fig. 4.6a, b) . Massive bone is drilled with a diamond burr or chiseled ; thin bony septa are broken or chopped. For preservation of the covering mucosa, preference is given to cutting forceps and punches (Fig. 4.7a, b) . Angled gripping instruments with which one can pack, cut, palpate, or displace particular areas of the sinus system are still being developed. The sets of instruments shown in Fig. 4.6 a, b are suitable,but do not represent the ideal, final solution. The experienced surgeon will be satisfied with a few slender instruments that lie easily in the hand and that with continuous practice allow all necessary dissection. The popular use of the ordinary Blakesley forceps in three different sizes is due to its slim and effective design with a tapering tip and tight mouth. It does not cut, however, but tends to tear the adherent mucosa. Double-cup forceps are less firm and also not sharp, but are indispensable, especially those with curved shafts, for grasping small polyps from remote areas. Punches are essential for bone work; their sharp cutting modifications are preferable. For the enlargement of small tunnels, the Bolger spoon curette (Fig. 4.8; see also Fig. 4.6a) and a diamond rasp have proved valuable. The shaver (Fig. 4.9) is favored by many rhinologists for the removal of polyps. It must be said, however, that thisabrasion is not always comparable to a thorough exenteration of the polyps’ roots but is limited to their gross reduction despite the ability of the shaver to abrade thin bony septa. The laser is also useful for special purposes (Fig. 4.10a, b) . Its domain is the inferior turbinate, which can be markedly reduced by stitch cautery, using a CO2 or Nd:Yag laser. A sharp wire sling is needed for the transaction of an occluding posterior tip.
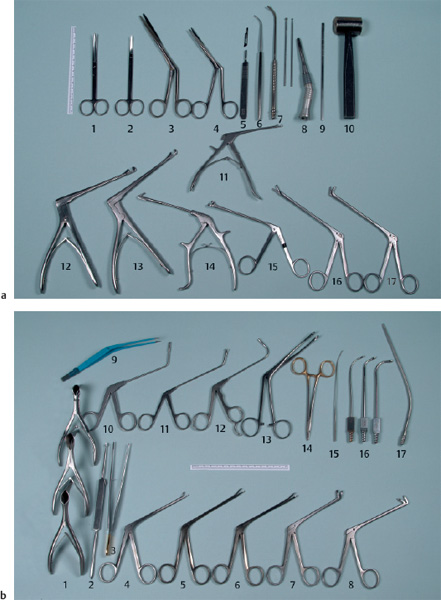
Fig. 4.6 a, b Standard set of instruments for endoscopic sinus surgery.
a Cutting instruments for severance of tissues.
1, Curved Joseph scissors;
2, straight pointed scissors;
3, superlong nasal scissors;
4, Heymann curved nasal scissors;
5, scalpel;
6, Kuhn–Bolger spoon curette 55°;
7, diamond rasp with suction device;
8, Portmann microdrill with diamond burrs;
9, Cottle chisel 4 mm;
10, Cottle mallet;
11, small 45° punch;
12, Hajek punch;
13, 45° punch;
14, Ostrom back-biting punch;
15, ring conchotome;
16, Wigand straight cutting forceps;
17, Wigand 45° cutting forceps.
b Instruments for dissection.
1, Hartmann nasal specula 3.5 cm, 5.5 cm, 7.5 cm;
2, Masing double-end dissector;
3, anatomical pincers, tungsten-coated 18.5 cm;
4–6, Blakesley nasal forceps sizes 0–2;
7, 8, Blakesley–Wilde nasal forceps 45° and 90°;
9, angled bipolar cautery forceps;
10, curved double-cup vertical forceps;
11, curved double-cup horizontal forceps;
12, 110° curved double-cup horizontal forceps;
13, Luc nasal ring forceps;
14, tungsten carbide needle holder;
15, curved cotton applicator;
16, sinus suction tubes 2.5 mm, 3.2 mm, 4.0 mm;
17, angled suction tube 3 mm.
For the precise coagulation of a bleeding artery, the bipolar cautery (Fig. 4.6b) is essential. Monopolar cautery can become necessary for tumor surgery. It is, however, always dangerous in the vicinity of nerves, important blood vessels, or the meninges.
Dissectors of various sizes (Fig. 4.6b) are available for various tasks such as blunt elevation of the dura from the bone or the mobilization of the periorbita. Sharp distraction of periosteum is necessary in external approaches. For the semisharp decollement of the nasal septum, the Masing dissector is optimal.
Suction tubes of different shapes and diameters are of great importance for cleaning the surgical field of blood and secretions (Fig. 4.6b) and for operative wound care.
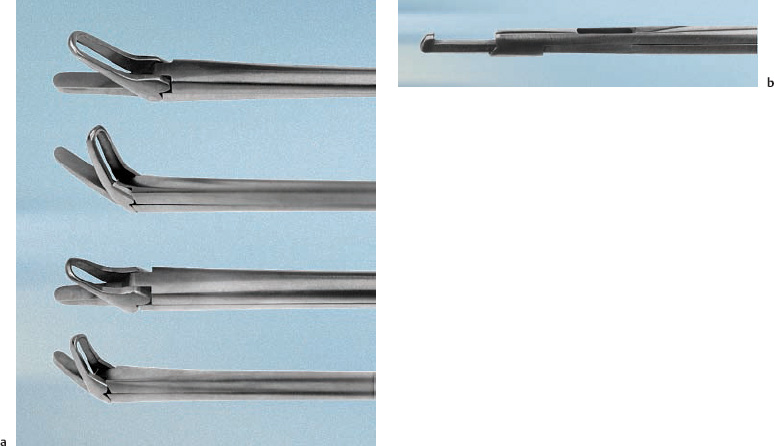
Fig. 4.7 a, b Cutting forceps and punch of the author.
a Cutting straight and 30° curved forceps (2.5 mm” 11.5 mm) with smaller modification (2 mm “ 6 mm) for pediatric ESS. The thin, rigid lower jaw is used as a perforator, while the mobile upper jaw is the cutting part.
b Through-cutting punch, 3 mm wide, with reservoir to pick up and collect bone material to be removed with a stylet (Stuemer–Gyrus instruments). Especially designed for sphenoid cavity wall resection.
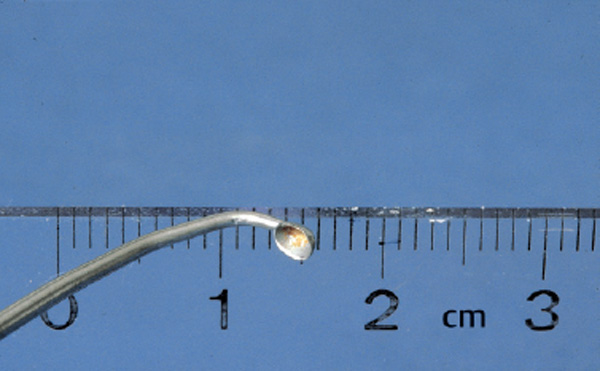
Fig. 4.8 Small cup curette of Bolger–House (cm scale).

Fig. 4.9 The powered shaver for endonasal combined aspiration and shearing of prominent soft tissue and thin bone.
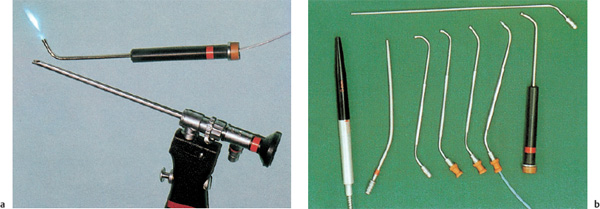
Fig. 4.10 a Principle of paraendoscopic argon laser surgery in the sinuses. A flexible cable in a curved tube is shown above, and below the suction–irrigation endoscope for optical monitoring. b Various curved introduction tubes for attaching flexible fibers for the use of the argon or Neodym: YAG laser in sinus surgery. A straight handpiece is shown on the left, and two straight, hollow tubes lie next to it and above.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


