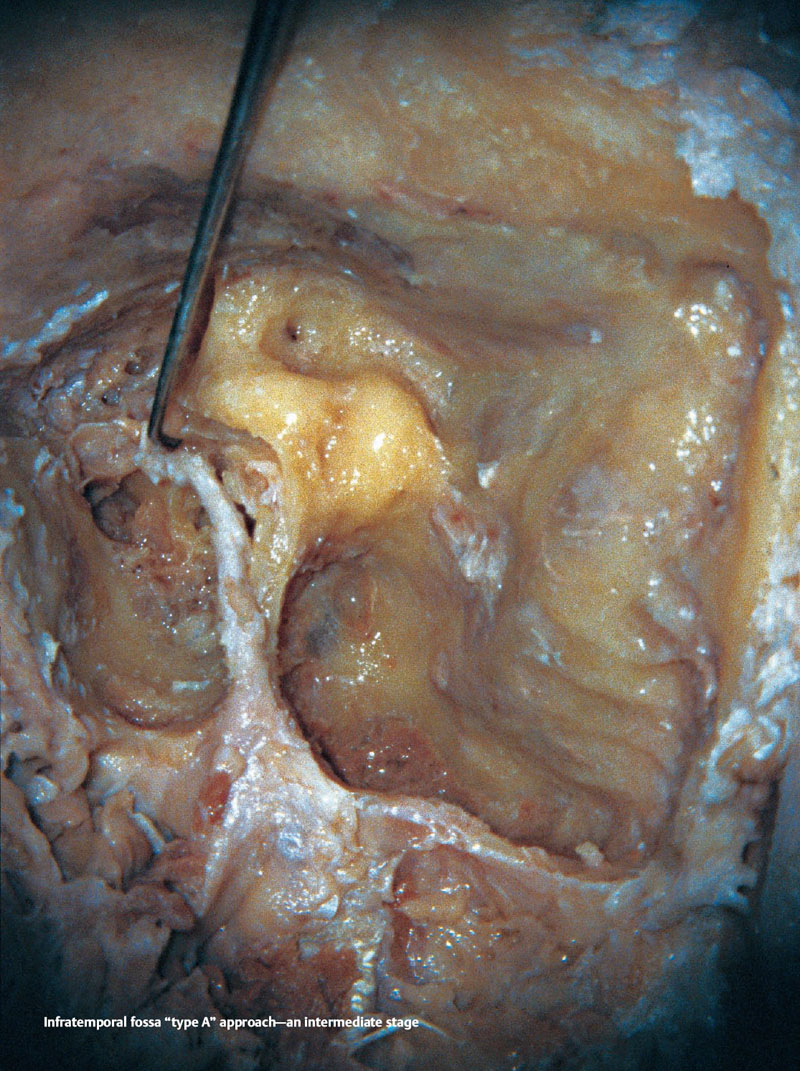
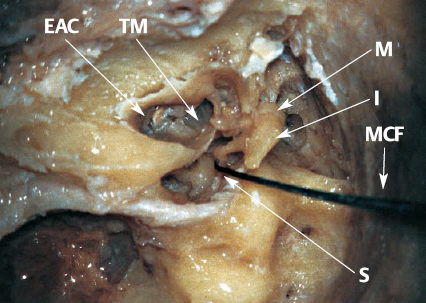
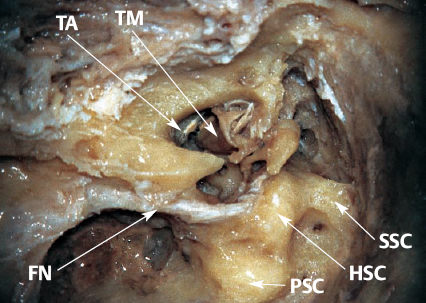
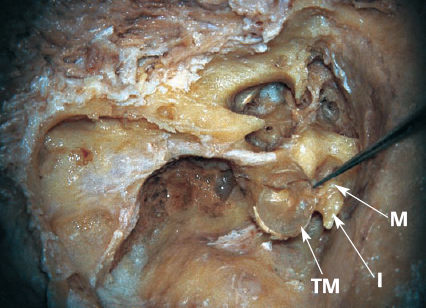
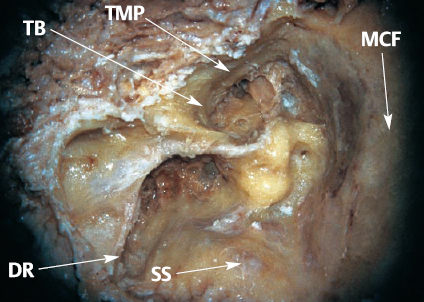
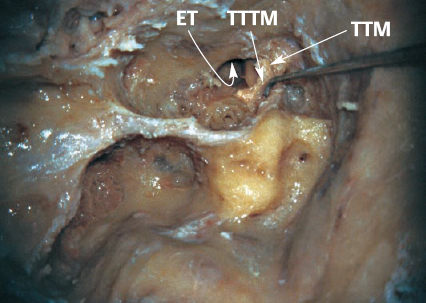
23 Infratemporal Fossa “Type A” Approach Following a subtotal petrosectomy, permanent anterior transposition of the facial nerve, and performing procedures on the structures located medial to the facial canal. At the end of this approach, abdominal fat is put into the cavity and a “blind sac” closure of the external auditory canal is carried out. An infratemporal fossa “type A” approach is mainly carried out for removal of glomus jugulare tumors and neuromas of cranial nerves IX–XII. The procedure will be carried out on the temporal bone where a modified radical mastoidectomy and exposure of the facial nerve have already been performed. In the first stage, the incudostapedial joint is separated with a micro hook. II: Micro hook MIL: Stapes head EAC: External auditory canal I: Incus M: Malleus MCF: Middle cranial fossa (dural plate) S: Stapes TM: Tympanic membrane The tympanic membrane is separated from the tympanic annulus by means of a micro elevator and positioned superiorly. The anatomical structures encountered during this stage are indicated in this and the previous figure. II: Micro elevator MIL: Tympanicannulus FN: Facial nerve HSC: Horizontal semicircular canal PSC: Posterior semicircular canal SSC: Superior semicircular canal TA: Tympanic annulus TM: Tympanic membrane After separating the tympanic membrane from the tympanic annulus circumferentially, and making a cut to the tendon of the tensor tympani muscle, the tympanic membrane, including the malleus and incus, is removed as a whole unit. I: Incus M: Malleus TM: Tympanic membrane Definitions and Tips II: 3–4mm cutting burr MIL: Facial nerve Drilling of the anterior part of the temporal bone is continued and the anterior wall of the tympanic bone is thinned until a bluish-pink discoloration indicates the temporomandibular joint reflection. Alternatively, the periosteum of the temporomandibular joint can be directly exposed, depending on the needs of the individual procedure. II: 3–4mm cutting and diamond burrs MIL: Temporomandibular joint periosteum DR: Digastric ridge MCF: Middle cranial fossa (dural plate) SS: Sigmoid sinus (dural plate) TB: Tympanic bone TMP: Temporomandibular joint periosteum (plate) Following this, the inferior part of the tympanic bone is drilled extensively. When working in this area, the blue-colored reflection of the jugular bulb should be sought, in both the laboratory and the operation. II: 3–4mm cutting and diamond burrs MIL: Jugular bulb reflection Definitions and Tips II: Curved micro dissector MIL: Cochleariform process ET: Eustachian tube TTM: Tensor tympani muscle TTTM: Tendon of tensor tympani muscle At this point, using medium-sized cutting and diamond burrs, the bone at the zygomatic root is drilled and a groove is made, beginning at the geniculate ganglion and ending at the squamosa. The facial nerve will later be transposed and placed into this groove. II: 2–3mm cutting and diamond burrs MIL: Geniculate ganglion This completes the subtotal petrosectomy, the full exposure of the facial nerve, and the creation of the “groove.” The figure shows a wide-angle view of the surgical site. In the operation, the extratemporal facial nerve trunk should be found, and its two main branches exposed in the parotid gland, prior to the execution of the aforementioned procedures.
Definition
Indications
Anatomical Orientation
Surgical Steps




Infratemporal Fossa “Type A” Approach
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


