Purpose
To evaluate the influence of the extent of myopia on the progression rate of normal-tension glaucoma (NTG).
Design
Retrospective, observational case series.
Methods
One hundred forty-three eyes of 143 patients with NTG who were treated from 1994 through 2006 and followed up with standard automated perimetry were evaluated in this study. The participants were divided into 4 groups: mild myopia (−0.76 to −2.99 diopters [D]), moderate myopia (−3 to −5.99 D), severe myopia (−6 D or less), and nonmyopia (emmetropia and hyperopia, −0.75 D or more) groups. The change in mean deviation, corrected pattern standard deviation, mean thresholds of 10 zones corresponding to the glaucoma hemifield test, and thresholds of 52 points of the nonmyopia group were compared with those of the other myopia groups. Additionally, we controlled each analysis for age and posttherapeutic intraocular pressure to preclude the possibility of these covariates influencing the analysis of the effect of myopia on the progression of glaucoma.
Results
There was no statistically significant difference between the nonmyopia group and each of the myopia groups in terms of mean deviation, corrected pattern standard deviation, mean thresholds of 10 zones corresponding to the glaucoma hemifield test, and the thresholds of 52 point changes against refraction. Moreover, with the control of the other covariates (age and posttherapeutic intraocular pressure), no statistically significant differences were noted (multivariate analysis using mixed model, P > .1).
Conclusions
Although a high incidence of open-angle glaucoma among myopic patients has been reported previously, myopia did not influence the progression rate of NTG after treatment.
The correlation between myopia and glaucoma has been a focus of interest in glaucoma research for a long time. Several studies already have proved the relatively high incidence rate of glaucoma in myopic patients. The Beaver Dam Eye Study reported that the incidence rate of glaucoma in myopic patients was 1.6 times higher than in those with emmetropia. The Malmo Eye Study reported that glaucoma developed in 1.5% of individuals with myopia and in 0.9% of those with emmetropia.
Thus, several explanations are possible. One of them asserts that myopia includes an anatomic weakness of the disc, which manifests as increased cup size, unusually large or skewed canal shape, and thin sclera and lamina in the disc periphery. Furthermore, reduced blood flow and low ocular pulse amplitude have been reported in myopic eyes. For these reasons, the optic disc in myopic patients may be subject to ischemia or damage at any level of intraocular pressure (IOP).
Although it has been demonstrated previously that myopia is associated with increased incidence of glaucoma, the effect of myopia on the progression of glaucoma has yet to be elucidated. Quigley and associates and Perkins and Phelps reported that visual field (VF) defects were observed more frequently in myopic patients with untreated ocular hypertension. Chihara and Sawada reported that myopia was a risk factor in the progression of POAG. However, Nouri-Mahdavi and associates and Phelps reported that myopia did not affect the progression of primary open-angle glaucoma (POAG) under treatment.
These previous studies simply assessed the progression or nonprogression of glaucoma, considering myopia as one of various risk factors. Additionally, no studies have been conducted yet regarding the progression rate of glaucoma in association with the degree of myopia, nor have any studies been conducted with the other risk factors being controlled. This study particularly evaluated the effect of myopia on the progression rate of normal-tension glaucoma (NTG) in an effort to answer the question as to whether myopia should be considered in the treatment or prognosis of NTG.
Methods
Study Subjects
Among 874 patients diagnosed with NTG at the Department of Ophthalmology of the Samsung Medical Center from 1994 through 2006 and who were treated only with a topical hypotensive agent, 143 ultimately were selected.
Inclusion criteria
In a retrospective study involving the records of 874 patients, 198 were selected for study based on the inclusion criteria described below. A diagnosis of NTG was made when a patient with an IOP of 21 mm Hg or less without treatment had findings of glaucomatous optic disc damage and corresponding VF defects, an open angle observed by gonioscopic examination, and no underlying cause for the optic disc damage aside from glaucoma. Each patient had to have been followed up in the outpatient clinic for 5 years or more and to have a VF test twice yearly, for a total of 10 or more VF tests. In patients with bilateral NTG, one eye was selected randomly and analyzed. Among 874 total subjects, 198 subjects were considered eligible.
Exclusion criteria
Among the 198 selected patients, we further excluded any patient with (1) another ocular disorder (11 patients), (2) any history of ocular surgery and laser including cataract surgery (21 patients), (3) lens opacities more severe than C2,N2,P2 according to lens opacities classification system III criteria (13 patients), and (4) visual acuity of less than 20/40 (10 patients). Besides cataract formation, we were particularly careful to consider factors such as large peripapillary atrophy and myopic maculopathy, both of which are common in patients with high myopia and can influence VF. We performed a careful fundus examination, stereo disc photography, retinal nerve fiber layer photos, and optical coherence tomography semiannually to observe for any myopic maculopathy or large peripapillary atrophy. If either of these two conditions developed, the subject then was excluded and these 4 patients were included in the fourth exclusion criterion, visual acuity of less than 20/40 (10 patients).
Treatment
When NTG was diagnosed, the patients received betaxolol 5 mg/mL (Alcon, Inc, Fort Worth, Texas, USA) twice daily. During the follow-up, if glaucoma progressed or did not reach the target IOP, betaxolol was replaced by latanoprost 50 μg/mL (Pfizer, Inc., New York, New York, USA).
The first target of IOP reduction was to reduce 30% of basal IOP. But if it did not reach its first target IOP, 14 mm Hg was set for the second target IOP. When latanoprost did not have sufficient effect, brimonidine 2 mg/mL (Allergan, Inc., Irvine, California, USA) usually was added.
A Goldmann applanation tonometer was used for IOP measurement. The basal IOP was calculated as the mean IOP of each hospital visit before the administration of a topical hypotensive agent. Additionally, the posttherapeutic IOP was calculated as the mean IOP of each hospital visit after the administration of a topical hypotensive agent.
Grading
Refractive status was measured via a manifest refraction test using a spherical equivalent. Emmetropia was defined as between −0.75 and 0.75 diopters (D) and hyperopia as 0.76 D or more. Myopia was classified into mild myopia (−0.76 to −2.99 D), moderate myopia (−3 to −5.99 D), and severe myopia (−6 D or less).
Visual Field Testing
The Central 30-2 full-threshold program of the Humphrey Visual Field Analyzer (Carl Zeiss Ophthalmic System, Inc., Dublin, California, USA) was used for VF testing. A reliable VF had to fulfill 3 criteria: fixation loss less than 20%, a false-positive rate of 30% or less, and a false-negative rate of 30% or less. The results of the first 2 tests were excluded to remove the learning effect from the final analysis. Additionally, those with a mean deviation (MD) of −25 dB or less, for whom glaucoma progression would be difficult to evaluate from a VF test, also were excluded. The corrected pattern standard deviation (CPSD) with mean deviation (MD) of −12 dB or less was excluded from the analysis, because the CPSD may be decreased when the glaucoma progresses to severe status. VF data for left eyes were switched across the vertical meridian such that, for example, the nasal area for the left eyes corresponded with the nasal area for the right eyes in all analyses. Hence, all figures of VF are presented as right eyes, although they actually represent mixed results from right and left eyes.
Using these VF results, the glaucoma progression rate and progression or nonprogression in myopic groups were analyzed statistically in comparison with those of the nonmyopic groups. The determination of time to progression is based on glaucoma change probability maps (GCPMs) of total deviation (TD), which is included in the STATpac software package of the Humphrey Visual Field Analyzer. To detect VF progression, all follow-up results of the VF tests were compared with an average of 2 baseline VF tests from the same eye using GCPMs. Definite VF progression was defined as at least 3 test points exhibiting significant ( P < .05) progression at the same locations on 3 consecutive tests as compared with the baseline.
Progression Rate Analysis
Univariate analysis
The first method used for comparisons of the progression rate was univariate analysis, using linear regression, which concerned only the effects of myopia. The progression rate of each myopic and nonmyopic group was calculated by linear regression. The methods of univariate analysis were as follows.
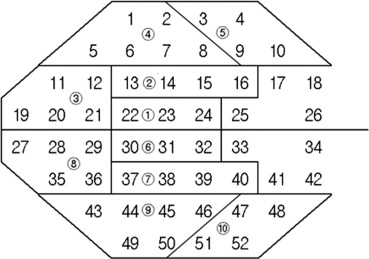
VF data (MD, CPSD, the thresholds of 52 points) were transferred to a personal computer, and univariate linear regression was conducted with time as the independent variable. Regression analysis was conducted with respect to 2 global indices (MD and CPSD), and similar analysis was conducted for the mean thresholds of the 10 zones corresponding to those of the glaucoma hemifield test and the thresholds of the 52 test points ( Figure 1 ). Sixty-four linear regressions (1(MD) + 1(CPSD) + 10(zones) + 52(points) = 64) were conducted for each individual.
Among them, the P ≤ .025 for the slope of the MD and CPSD, P ≤ .005 for the slope of 10 zones, and P ≤ .001 for the slope of 52 points were considered to be statistically significant. Only such significant values were selected for the calculation of the mean values of the progression rate.
Multivariate analysis
The second method used for the comparison of the progression rate was a multivariate analysis using a mixed model. Each progression rate of MD, CPSD, 10 zones, and 52 points over time was compared by multivariate analysis using the mixed model between the myopia and nonmyopia groups. Multivariate analysis was used to evaluate the association of the continuous dependent variable of the degree of myopia (each myopic and non-myopic groups) with the binary independent variable of progression rate.
Additionally, covariates including age, sex, diabetes mellitus (DM), hypertension (HTN), basal IOP, posttherapeutic IOP, basal MD, and basal CPSD were controlled using various covariate combinations. Thus, 64 (1(MD) + 1(CPSD) + 10(zones) + 52(point)) times of multivariate analyses using a mixed model were conducted with each covariate combination; therefore, more than hundreds of analyses were conducted in total.
Survival analysis
The third method used for comparisons of the progression rate was Kaplan-Meier survival analysis of time to progression. The process of the progression decision was the same as the above explanations using GCPMs of TD.
Progression or Nonprogression Analysis
Univariate analysis
The final method used in this study was used to compare progression or nonprogression, and not the aforementioned progression rate. The decision-making process for progression is the same as explained above, using GCPMs of TD. The Student t test was used to analyze the degree of myopia between the progression and nonprogression groups, and a chi-square test was used to analyze the differences in the frequency of progression between the myopic and nonmyopic groups.
Multivariate analysis
Additionally, using logistic regression, the association of VF progression with myopia was evaluated, and the influences of age and posttherapeutic IOP were explored. All statistical analyses were conducted using SAS software version 8.0 (SAS, Inc., Cary, North Carolina, USA) and SPSS software version 11.0 (SPSS, Inc., Chicago, Illinois, USA).
Results
General Analysis
Among 874 patients, 143 patients and 143 eyes (67 from males and 76 from females) fulfilled the inclusion criteria of this study. With regard to the classification of refractive error, (1) 22 eyes were categorized with mild myopia (−0.76 to −2.99 D), (2) 22 eyes with moderate myopia (−3 to −5.99 D), and (3) 24 eyes with severe myopia (−6 D or less). In the 75 nonmyopic eyes (−0.75 D or more), (1) 51 eyes were categorized with emmetropia (−0.75 to 0.75 D) and (2) 24 eyes with hyperopia (0.76 D or more). Age, refraction, basal IOP, posttherapeutic IOP, frequency of VF testing, basal MD, basal CPSD, and follow-up period for each group are listed in Table 1 . Except for the refraction value, there were no significant differences in any variable used in comparisons between the nonmyopic group and any of the myopic groups.
| Characteristics | Nonmyopic Group (Hyperopia and Emmetropia −0.75 D or more; n = 75) | Mild Myopia Group (−0.76 to −2.99 D; n = 22) | Moderate Myopia Group (−3 to −5.99 D; n = 22) | Severe Myopic Group (−6 D or less; n = 24) | P Value a |
|---|---|---|---|---|---|
| Age | 61.8 ± 8.9 | 59.7 ± 10.8 | 65.5 ± 10.5 | 60.7 ± 8.6 | .624 |
| Sex (male/female) | 35/40 | 8/14 | 7/15 | 17/7 | .230 |
| Refraction (D) | 0.39 ± 0.75 | −1.92 ± 0.55 | −4.57 ± 0.76 | −9.37 ± 0.43 | 0 |
| Basal IOP (mm Hg) | 16.1 ± 2.4 | 17.7 ± 2.5 | 17.1 ± 2.9 | 16.9 ± 3.2 | .131 |
| Posttherapeutic IOP (mm Hg) | 14.4 ± 1.9 | 14.8 ± 2.0 | 15.1 ± 1.8 | 15.0 ± 1.9 | .419 |
| Ratio of IOP lowering (%) | 13.2 ± 7.3 | 14.8 ± 8.4 | 14.2 ± 8.9 | 13.6 ± 6.8 | .517 |
| No. of examinations | 8.4 ± 3.1 | 8 ± 2.7 | 9.2 ± 3.6 | 9.5 ± 3.6 | .307 |
| Basal MD (dB) | −6.7 ± 4.9 | −6.7 ± 4.1 | −7.1 ± 5.0 | −7.1 ± 5.4 | .665 |
| Basal CPSD (dB) | 6.9 ± 4.1 | 7.5 ± 3.6 | 8.5 ± 4.9 | 7.1 ± 3.6 | .524 |
| Follow-up (mos) | 67.4 ± 21.6 | 63.8 ± 23.5 | 67.7 ± 25.0 | 69.4 ± 24.3 | .865 |
| Diabetes mellitus (n) b | 10 | 5 | 3 | 3 | .957 |
| Hypertension (n) c | 13 | 3 | 4 | 4 | .975 |
c Defined as systolic pressure more than 160 mm Hg, diastolic pressure more than 95 mm Hg, or medical history.
Progression Rate Analysis
Univariate and multivariate analysis
Changes in the linear regression values for MD for each group were as follows: −1.334 dB/year for the nonmyopic group and −1.055 dB/year, −1.113 dB/year, and −0.912 dB/year for the mild, moderate, and severe myopic groups, respectively. Results of multivariate analysis using the mixed model, in which age and posttherapeutic IOP were controlled, revealed no statistically significant differences between groups ( P = .255).
The change in the CPSD by linear regression analysis in the nonmyopic group was 0.967 dB/year and 1.525 dB/year, 1.022 dB/year, and 1.259 dB/year for the mild, moderate, and severe myopic groups, respectively. There was no significant between-group differences by multivariate analysis using the mixed model ( P = .106; Table 2 ).
| Nonmyopic Group | Mild Myopia Group | Moderate Myopia Group | Severe Myopia Group | P Value a | |
|---|---|---|---|---|---|
| MD (dB/year) | −1.334 ± 1.003 | −1.055 ± 0.328 | −1.113 ± 0.466 | −0.912 ± 0.313 | .255 |
| CPSD (dB/year) | 0.967 ± 0.48 | 1.525 ± 0.7 | 1.022 ± 0.126 | 1.259 ± 0.748 | .106 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


