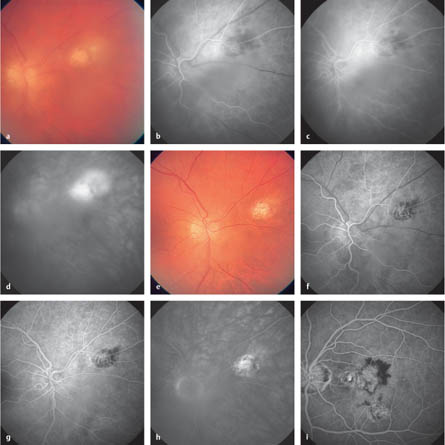
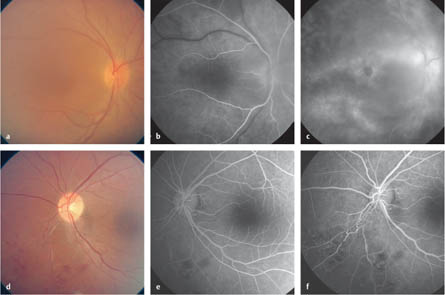
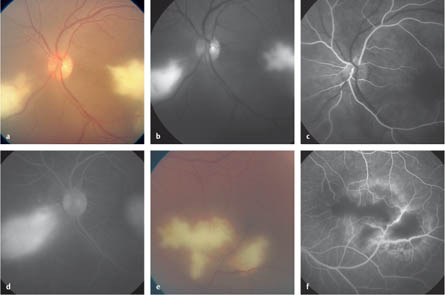
9.1 Toxoplasmosis Chorioretinitis Bosch-Driessen LE, Berendschot TT, Ongkosuwito JV, Rothova A. Ocular toxoplasmosis: clinical features and prognosis of 154 patients. Ophthalmology 2002;109:869–78. Holland GN. Ocular toxoplasmosis: new directions for clinical investigation. Ocul Immunol Inflamm 2000;8:1–7. Holland GN, Lewis KG. An update on current practices in the management of ocular toxoplasmosis. Am J Ophthalmol 2002;134: 102–14. Mets MB, Holfels E, Boyer KM, et al. Eye manifestations of congenital toxoplasmosis. Am J Ophthalmol 1996;122:309–24. Rothova A. Ocular manifestations of toxoplasmosis. Curr Opin Ophthalmol 2003;14:384–8. Fig. 9.1a–i Toxoplasmosis chorioretinitis a Color photograph. At the upper temporal vessels, a whitish scar with a fleecy, inflammatory infiltrate directly adjacent to the scar is visible. The view of the fundus is restricted due to an inflammatory vitreous infiltrate. b Early phase. Hypofluorescence in the scar area and hyperfluorescence in the acute inflamed area are visible. c Arteriovenous phase. Incipient leakage in the border area of the scar and in the infiltrate. d Late phase. The leakage is continuing to decrease in the scar area, as well as in the area of the fresh infiltrate. e Color photograph. After 8 weeks of healing of the inflammatory lesion, only a scar with retinal pigment epithelial irregularities remains. There is also noticeably better visualization of the fundus. f Early phase. Improved visibility of choroidal filling in the area of the scar. g Arteriovenous phase. Limited hyperfluorescence in the border region of the scar. h Late phase. The hyperfluorescence remains unchanged in the scar area. i Arteriovenous phase (in a different patient). Choroidal neovascularization has developed at the border of a toxoplasmosis scar as a complication of the damage to the integrity of the retina, retinal pigment epithelium, and choroid. Atmaca LS, Batioglu F, Idil A. Retinal and disc neovascularization in Behçet’s disease and efficacy of laser photocoagulation. Graefes Arch Clin Exp Ophthalmol 1996;234:94–9. Bozzoni-Pantaleoni F, Gharbiya M, Pirraglia MP, Accorinti M, PivettiPezzi P. Indocyanine green angiographic findings in Behçet disease. Retina 2001;21:230–6. Matsuo T, Sato Y, Shiraga F, Shiragami C, Tsuchida Y. Choroidal abnormalities in Behçet disease observed by simultaneous indocyanine green and fluorescein angiography with scanning laser ophthalmoscopy. Ophthalmology 1999;106:295–300. Stanga PE, Lim JI, Hamilton P. Indocyanine green angiography in chorioretinal diseases: indications and interpretation: an evidence-based update. Ophthalmology 2003;110:15–21. Zouboulis CC. Epidemiology of Adamantiades–Behcet’s disease. Ann Med Interne (Paris) 1999;150:488–98. Fig. 9.2a–f Behçet disease a Color photograph. A patient with acute inflammation in confirmed Behçet disease. The visibility of the fundus is reduced due to the inflammatory vitreous infiltrate. The macula reflex has ceased; the optic disc is lightly hyperemic. b Early arteriovenous phase. There are discrete areas of hyper-fluorescence in the paramacular area as a sign of increased permeability due to inflammation. c Late phase. Cystoid macular edema is clearly recognizable by the parafoveal hyperfluorescence. Further areas of hyperfluorescence are visible along the temporal vessels. d Color photograph. Dot hemorrhages, vessel occlusion, and retinal edema in the nasal lower quadrant in acute vasculitis in the context of Behçet disease. e Arteriovenous phase. The areas of hemorrhage appear as blockage phenomena, and vascular wall irregularities are also visible. The avascular nasal lower sector appears hypofluorescent. f Late phase. Telangiectatic vessel changes in the nasal lower quadrant. The avascular area is still hypofluorescent. Laser coagulation in the affected quadrants should be considered. Cassoux N, Bodaghi B, Katlama C, LeHoang P. CMV retinitis in the era of HAART. Ocul Immunol Inflamm 1999;7:231–5. Cytomegalovirus (CMV) culture results, drug resistance, and clinical outcome in patients with AIDS and CMV retinitis treated with foscarnet or ganciclovir. Studies of Ocular Complications of AIDS (SOCA) in collaboration with the AIDS Clinical Trial Group. J Infect Dis 1997;176:50–8. Dhillon B, Ramaesh K, Leen C. Changing trends in cytomegalovirus retinitis with highly active anti-retroviral therapy (HAART). Eye 1999;13:275–6. Goldberg DE, Wang H, Azen SP, Freeman WR. Long term visual outcome of patients with cytomegalovirus retinitis treated with highly active antiretroviral therapy. Br J Ophthalmol 2003;87: 853–5. Ritterband DC, Friedberg DN. Virus infections of the eye. Rev Med Virol 1998;8:187–201. Tran TH, Stenescu D, Caspers-Velu L, et al. Clinical characteristics of acute HSCV-2 retinal necrosis. Am J Ophthalmol 2004;137:872–9. Fig. 9.3a–f Cytomegalovirus and herpes simplex virus retinitis a Color photograph. Acute cytomegalovirus retinitis with white infiltrates located nasal and temporal to the optic disc. A vessel in the area of the nasal scars has been destroyed. The view of the fundus is reduced by cellular vitreous body infiltration. b Black and white photograph. There are retinal infiltrates nasal and temporal to the optic disc. c Early arteriovenous phase. There are occluded vessels in the area of the nasal infiltrates; otherwise, regular arterial filling can be seen. A filling defect is also visible in the choroid in the area of the nasal infiltrates. d Late phase. Hyperfluorescence in the infiltrated area as an expression of increased leakage. e Color photograph. There is a retinal infiltrate in the temporal area and vascular lesions are also present in the area of the inflamed retina. f Arteriovenous phase. There is a filling defect (hypofluorescence) in the infiltrated area. Incipient hyperfluorescence is visible at the border of the lesion. Vascular wall irregularities and leakage from the vessels damaged by inflammation are recognizable.
Epidemiology, Pathophysiology, and Clinical Presentation
 Toxoplasma gondii is the pathogen involved in the most common form of posterior uveitis. The infection is mainly congenitally acquired, and a scar often develops in the macular region. However, the disease can also arise in the context of postnatal toxoplasmosis infection.
Toxoplasma gondii is the pathogen involved in the most common form of posterior uveitis. The infection is mainly congenitally acquired, and a scar often develops in the macular region. However, the disease can also arise in the context of postnatal toxoplasmosis infection.
 The pathogen persists in an encapsulated form in the cells. Reactivation of the pathogen can occur, and an inflammatory reaction then often appears on the edge of an old postinflammatory scar.
The pathogen persists in an encapsulated form in the cells. Reactivation of the pathogen can occur, and an inflammatory reaction then often appears on the edge of an old postinflammatory scar.
 On ophthalmoscopy, a yellow-white, somewhat unclear, limited retinal or chorioretinal lesion is visible, sometimes with a distinct vitreous body infiltration, which leads to a restricted view of the fundus. The acute lesions are mainly located at the posterior pole of the eye.
On ophthalmoscopy, a yellow-white, somewhat unclear, limited retinal or chorioretinal lesion is visible, sometimes with a distinct vitreous body infiltration, which leads to a restricted view of the fundus. The acute lesions are mainly located at the posterior pole of the eye.
 An immediate juxtapapillary position (Jensen) represents a special form. A curved scotoma typically forms as a result.
An immediate juxtapapillary position (Jensen) represents a special form. A curved scotoma typically forms as a result.
 Choroidal neovascularization is a rare complication.
Choroidal neovascularization is a rare complication.
Fluorescein Angiography
 Fluorescein angiography is not generally necessary for diagnosis of toxoplasmosis chorioretinitis, but in certain cases it is helpful in the differential diagnosis.
Fluorescein angiography is not generally necessary for diagnosis of toxoplasmosis chorioretinitis, but in certain cases it is helpful in the differential diagnosis.
 In the early phase, hypofluorescence appears in the area of the old scars, and the fresh infiltrate shows hyperfluorescence as a sign of increased leakage.
In the early phase, hypofluorescence appears in the area of the old scars, and the fresh infiltrate shows hyperfluorescence as a sign of increased leakage.
 The arteriovenous phase shows diffuse hyperfluorescence in the area of the infiltrates, and hypofluorescence appears in the region of the scars.
The arteriovenous phase shows diffuse hyperfluorescence in the area of the infiltrates, and hypofluorescence appears in the region of the scars.
 In the late phase, there is an increase in the hyper-fluorescence, indicating increasing leakage.
In the late phase, there is an increase in the hyper-fluorescence, indicating increasing leakage.
Diagnosis and Treatment
 The diagnosis is based on the ophthalmoscopic findings. Obtaining serological evidence from blood samples is often difficult. In case of uncertainty, material for a polymerase chain reaction (PCR) diagnosis can be extracted by aspirating fluid from the anterior chamber.
The diagnosis is based on the ophthalmoscopic findings. Obtaining serological evidence from blood samples is often difficult. In case of uncertainty, material for a polymerase chain reaction (PCR) diagnosis can be extracted by aspirating fluid from the anterior chamber.
 The functional prognosis depends on the location of the infiltrate, with proximity to the fovea and the optic disc being the decisive aspect.
The functional prognosis depends on the location of the infiltrate, with proximity to the fovea and the optic disc being the decisive aspect.
 Vasculitis, vascular occlusion, and active infiltrates can be confirmed with fluorescein angiography. Choroidal neovascularizations, as a possible complication, can also be demonstrated with this method.
Vasculitis, vascular occlusion, and active infiltrates can be confirmed with fluorescein angiography. Choroidal neovascularizations, as a possible complication, can also be demonstrated with this method.
 The indications for treatment vary widely. Treatment of lesions that are at a considerable distance from the optic disc and macula is not necessary, as the acute disease is self-limiting and treatment of the encapsulated form dormant in the cells is not possible.
The indications for treatment vary widely. Treatment of lesions that are at a considerable distance from the optic disc and macula is not necessary, as the acute disease is self-limiting and treatment of the encapsulated form dormant in the cells is not possible.
 Treatment is required in cases in which there is an infiltration near the macular region or the optic disc. Various combinations of treatments have been described. A combination of sulfadiazine and pyrimethamine is the most common form of therapy at present (with additional systematic corticosteroid administration after an interval of 2 days).
Treatment is required in cases in which there is an infiltration near the macular region or the optic disc. Various combinations of treatments have been described. A combination of sulfadiazine and pyrimethamine is the most common form of therapy at present (with additional systematic corticosteroid administration after an interval of 2 days).
 Clindamycin treatment is also effective, but pseudo-membranous colitis can occur as a side effect in some cases.
Clindamycin treatment is also effective, but pseudo-membranous colitis can occur as a side effect in some cases.
 If choroidal neovascularization develops, treatment similar to the established regimens in age-related macular degeneration is recommended.
If choroidal neovascularization develops, treatment similar to the established regimens in age-related macular degeneration is recommended.
References
9.2 Behçet Disease
Epidemiology, Pathophysiology, and Clinical Presentation
 Behçet disease is a generalized vasculitis, with skin and mucous membrane involvement (oral and genital ulcers). The etiology is unclear, but there is probably a multifactorial pathogenesis involved a particular HLA disposition (HLA-B51) and triggering of the immune system caused by an unknown pathogen.
Behçet disease is a generalized vasculitis, with skin and mucous membrane involvement (oral and genital ulcers). The etiology is unclear, but there is probably a multifactorial pathogenesis involved a particular HLA disposition (HLA-B51) and triggering of the immune system caused by an unknown pathogen.
 Occurrences are particularly common in Asian countries.
Occurrences are particularly common in Asian countries.
 The retinal and choroidal vessels may be involved if there is ophthalmic involvement. Simultaneous appearance of iritis and anterior uveitis is common, but not obligatory. Hypopyon may also be present.
The retinal and choroidal vessels may be involved if there is ophthalmic involvement. Simultaneous appearance of iritis and anterior uveitis is common, but not obligatory. Hypopyon may also be present.
 Vasculitis can be found in the retina with inflammatory perivascular infiltrates and retinal hemorrhages. Vascular occlusions accompanied by ischemic areas and subsequent development of neovascularizations and secondary glaucoma can also arise.
Vasculitis can be found in the retina with inflammatory perivascular infiltrates and retinal hemorrhages. Vascular occlusions accompanied by ischemic areas and subsequent development of neovascularizations and secondary glaucoma can also arise.
 Acute inflammatory macular edema can progress to chronic cystoid macular edema.
Acute inflammatory macular edema can progress to chronic cystoid macular edema.
 When there is optic disc involvement, swelling of the optic disc and peripapillary hemorrhage can arise, leading to optic atrophy.
When there is optic disc involvement, swelling of the optic disc and peripapillary hemorrhage can arise, leading to optic atrophy.
Fluorescein Angiography
 Fluorescein angiography is helpful in showing the extent of the retinal ischemic areas, from mild leakages emerging from affected vessels and cystoid macular edema.
Fluorescein angiography is helpful in showing the extent of the retinal ischemic areas, from mild leakages emerging from affected vessels and cystoid macular edema.
 Areas of hypofluorescence in the capillary occlusion area can be seen in the early phase, as well as ischemic areas and vessel wall irregularities.
Areas of hypofluorescence in the capillary occlusion area can be seen in the early phase, as well as ischemic areas and vessel wall irregularities.
 Areas of hyperfluorescence develop along the vessels in the arteriovenous phase due to increased permeability (involving both the arteries and the veins). Vascular occlusion and blockage of the choroidal fluorescence due to retinal and preretinal hemorrhages can be observed.
Areas of hyperfluorescence develop along the vessels in the arteriovenous phase due to increased permeability (involving both the arteries and the veins). Vascular occlusion and blockage of the choroidal fluorescence due to retinal and preretinal hemorrhages can be observed.
 In the late phase, hyperfluorescence intensifies due to increasing leakage, and cystoid macular edema may also become evident.
In the late phase, hyperfluorescence intensifies due to increasing leakage, and cystoid macular edema may also become evident.
Indocyanine Green Angiography
 Indocyanine green angiography can detect additional choroidal abnormalities, particularly hypofluorescent choroidal areas after a long duration of the disease.
Indocyanine green angiography can detect additional choroidal abnormalities, particularly hypofluorescent choroidal areas after a long duration of the disease.
 The clinical relevance of these findings is questionable.
The clinical relevance of these findings is questionable.
Diagnosis and Treatment
 The diagnosis is established in accordance with the criteria set out by the International Study Group for Behçet Disease: recurrent oral aphthae, plus at least two subcriteria (recurrent genital aphthae, ophthalmic involvement, skin involvement, or positive pathergy phenomenon).
The diagnosis is established in accordance with the criteria set out by the International Study Group for Behçet Disease: recurrent oral aphthae, plus at least two subcriteria (recurrent genital aphthae, ophthalmic involvement, skin involvement, or positive pathergy phenomenon).
 Evidence of vasculitis, vessel occlusion, ischemic areas, capillary occlusion, and cystoid macular edema can be provided by fluorescein angiography (see also Fig. 7.5 g–i).
Evidence of vasculitis, vessel occlusion, ischemic areas, capillary occlusion, and cystoid macular edema can be provided by fluorescein angiography (see also Fig. 7.5 g–i).
 The treatment for ophthalmic involvement in Behçet disease includes local and/or systemic corticosteroids and immunosuppressive agents (cyclosporine, azathioprine) as basic medication to reduce the frequency of relapses.
The treatment for ophthalmic involvement in Behçet disease includes local and/or systemic corticosteroids and immunosuppressive agents (cyclosporine, azathioprine) as basic medication to reduce the frequency of relapses.
 More recent research results have shown that the disease responds well to interferon-alpha and anti-tumor necrosis factor antibodies.
More recent research results have shown that the disease responds well to interferon-alpha and anti-tumor necrosis factor antibodies.
References
9.3 Cytomegalovirus and Herpes Simplex Virus Retinitis
Cytomegalovirus Retinitis
Epidemiology, Pathophysiology, and Clinical Presentation
 Congenital cytomegalovirus transmission usually leads to a subclinical disease course. In the affected children, the illness can cause conditions ranging from hearing defects to mental retardation. The retina is involved in approximately 30% of cases.
Congenital cytomegalovirus transmission usually leads to a subclinical disease course. In the affected children, the illness can cause conditions ranging from hearing defects to mental retardation. The retina is involved in approximately 30% of cases.
 The acquired form of cytomegalovirus retinitis generally appears in patients receiving treatment with immunosuppressive agents and in those with acquired immune deficiency syndrome (AIDS).
The acquired form of cytomegalovirus retinitis generally appears in patients receiving treatment with immunosuppressive agents and in those with acquired immune deficiency syndrome (AIDS).
 The retinitis is characterized by fluffy white retinal lesions (retinal necroses), vessel occlusions, and retinal hemorrhages.
The retinitis is characterized by fluffy white retinal lesions (retinal necroses), vessel occlusions, and retinal hemorrhages.
 The retinal necroses may be extensive, and retinal detachment may occur during the course of the disease. The inflammation usually leaves behind large areas of scarring with pigment changes.
The retinal necroses may be extensive, and retinal detachment may occur during the course of the disease. The inflammation usually leaves behind large areas of scarring with pigment changes.
Fluorescein Angiography
 Fluorescein angiography is generally not required for diagnosis.
Fluorescein angiography is generally not required for diagnosis.
 Blockage phenomena develop in the early phase in the area of the hemorrhages; otherwise, proper arterial filling takes place. Vessel irregularities may occur in the affected regions.
Blockage phenomena develop in the early phase in the area of the hemorrhages; otherwise, proper arterial filling takes place. Vessel irregularities may occur in the affected regions.
 The arteriovenous phase shows diffuse hyperfluorescence in the area of the vessels involved and infiltrates, as well as areas of hypofluorescence due to the avascular areas.
The arteriovenous phase shows diffuse hyperfluorescence in the area of the vessels involved and infiltrates, as well as areas of hypofluorescence due to the avascular areas.
 In the late phase, the areas of hyperfluorescence increase due to stronger and increasing leakage in the area of the inflamed vessels and possibly also in the optic disc area.
In the late phase, the areas of hyperfluorescence increase due to stronger and increasing leakage in the area of the inflamed vessels and possibly also in the optic disc area.
Diagnosis and Treatment
 The diagnosis is established by the ophthalmoscopic findings and the diagnostic pattern of the general findings.
The diagnosis is established by the ophthalmoscopic findings and the diagnostic pattern of the general findings.
 Currently, treatment consists of systematic administration of foscarnet or ganciclovir, possibly in combination with a vitreal ganciclovir implant. Therapy for possible AIDS is carried out in parallel.
Currently, treatment consists of systematic administration of foscarnet or ganciclovir, possibly in combination with a vitreal ganciclovir implant. Therapy for possible AIDS is carried out in parallel.
 After healing of the infection, the disease course may be complicated by reactivation of the infection, or in the longer term by epiretinal gliosis, cystoid macular edema, or retinal detachment. In these cases, vitrectomy may be indicated in some circumstances.
After healing of the infection, the disease course may be complicated by reactivation of the infection, or in the longer term by epiretinal gliosis, cystoid macular edema, or retinal detachment. In these cases, vitrectomy may be indicated in some circumstances.
Herpes Simplex Virus Retinitis
Epidemiology, Pathophysiology, and Clinical Presentation
 Herpes simplex virus can also be acquired either congenitally or later on. Ophthalmic involvement can lead to conjunctivitis, keratitis, or chorioretinitis. The pathogens are herpes simplex virus types I or II.
Herpes simplex virus can also be acquired either congenitally or later on. Ophthalmic involvement can lead to conjunctivitis, keratitis, or chorioretinitis. The pathogens are herpes simplex virus types I or II.
 Acute retinal necrosis in otherwise healthy individuals can occur when there is retinal involvement.
Acute retinal necrosis in otherwise healthy individuals can occur when there is retinal involvement.
 This is characterized by extensive retinal necroses and vessel obliterations; retinal detachment may develop during the course of the disease.
This is characterized by extensive retinal necroses and vessel obliterations; retinal detachment may develop during the course of the disease.
Fluorescein Angiography
 Fluorescein angiography is not generally necessary for diagnosis.
Fluorescein angiography is not generally necessary for diagnosis.
 In the early phase, areas of hypofluorescence develop due to retinal and choroid vessel occlusions.
In the early phase, areas of hypofluorescence develop due to retinal and choroid vessel occlusions.
 In the arteriovenous phase, leakages develop in the area of the inflamed vessels, and hyperfluorescence in areas with edema. Hypofluorescence develops in ischemic areas and due to blockages caused by hemorrhage.
In the arteriovenous phase, leakages develop in the area of the inflamed vessels, and hyperfluorescence in areas with edema. Hypofluorescence develops in ischemic areas and due to blockages caused by hemorrhage.
 In the late phase, increased leakage is observed.
In the late phase, increased leakage is observed.
Diagnosis and Treatment
 The diagnosis is based on the ophthalmoscopic findings.
The diagnosis is based on the ophthalmoscopic findings.
 Treatment consists of systemic administration of acyclovir and vitreoretinal surgery if appropriate.
Treatment consists of systemic administration of acyclovir and vitreoretinal surgery if appropriate.
References
9.4 Sarcoidosis
Epidemiology, Pathophysiology, and Clinical Presentation
 Sarcoidosis is a granulomatosis systemic disease, histopathologically characterized by noncaseating epithelial cellular granulomas with Langerhans giant cells. All inflammatory changes in the posterior eye should be included in the differential diagnosis of the disease.
Sarcoidosis is a granulomatosis systemic disease, histopathologically characterized by noncaseating epithelial cellular granulomas with Langerhans giant cells. All inflammatory changes in the posterior eye should be included in the differential diagnosis of the disease.
 The etiology of sarcoidosis is not known. The disease appears most frequently in the African-American population in the USA.
The etiology of sarcoidosis is not known. The disease appears most frequently in the African-American population in the USA.
 In over 90% of cases, the disease becomes manifest in the lung (with swelling of the hilar lymph nodes), but all of the other organs can be affected in the acute or chronic forms.
In over 90% of cases, the disease becomes manifest in the lung (with swelling of the hilar lymph nodes), but all of the other organs can be affected in the acute or chronic forms.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


