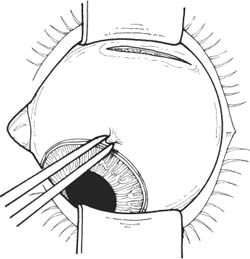
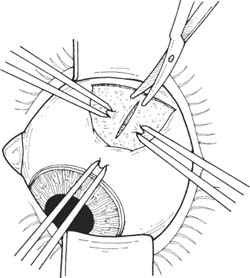
39 Inferior oblique muscle overaction requiring muscle weakening for correction, or concomitant dissociated vertical deviation requiring anterior transposition of the inferior oblique. See Chapter 3. A complete strabismus evaluation with determination of the detailed surgical plan is necessary. Note: Figures are drawn from the surgeon’s viewpoint with the surgeon standing at the head of the patient. Note: Illumination of the surgical field is best obtained with a headlight. 1. Anesthesia: General anesthesia or retrobulbar/peribulbar injection plus eyelid block. 2. Place a drop of neosynephrine 2.5% into the eye to constrict the blood vessels and decrease bleeding. Prep and drape. 3. Place lid speculum. Figure 39.1 4. Create conjunctival incision in the inferotemporal fornix (Fig. 39.1). a. The assistant grasps the globe at the limbus at the inferotemporal limbus. b. The assistant then exposes the inferior fornix by elevating and adducting the globe. c. Create an 8 mm incision parallel to the fornix and 1 mm from the fornix on the bulbar conjunctiva with Westcott scissors. Figure 39.2 5. Create a radial incision through the Tenon capsule to expose the sclera (Fig. 39.2). a. The assistant and surgeon grasp the Tenon capsule less than 10 mm from the limbus. b. Cut the Tenon capsule between the forceps and radially toward the limbus. c. The incision should reach bare sclera. If layers of Tenon capsule remain, repeat steps 5a-b. d. The incision should not extend more than 10 mm from the limbus or else orbital fat may be exposed and adherence syndrome may occur. 6. Isolate the lateral rectus with a Stevens hook.
Inferior Oblique Recession/Anterior Transposition
Indications
Preoperative Procedure
Instrumentation
 Lid speculum (e.g., Lancaster, Barraquer)
Lid speculum (e.g., Lancaster, Barraquer)
 Needle holder
Needle holder
 Sutures (4–0 silk suture, double-armed 6–0 Vicryl with spatula needle, 7–0 Vicryl suture)
Sutures (4–0 silk suture, double-armed 6–0 Vicryl with spatula needle, 7–0 Vicryl suture)
 Toothed forceps (e.g., Bishop-Harmon, 0.5 mm Castro-viejo)
Toothed forceps (e.g., Bishop-Harmon, 0.5 mm Castro-viejo)
 Westcott scissors (rounded tips)
Westcott scissors (rounded tips)
 Cautery (bipolar forceps)
Cautery (bipolar forceps)
 Muscle hook (e.g., Green, Jameson)
Muscle hook (e.g., Green, Jameson)
 Gass muscle hook
Gass muscle hook
 Stevens tenotomy hooks
Stevens tenotomy hooks
 Iris spatula
Iris spatula
 Hartman mosquito hemostat
Hartman mosquito hemostat
 Desmarres retractor
Desmarres retractor
 Castroviejo caliper
Castroviejo caliper
 Headlight
Headlight
Operative Procedure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


