Infections of the Salivary Glands
Vinidh Paleri
Introduction
Both bacteriae and viruses are involved in salivary gland infections. The clinical setting and clinical features do permit differentiation with a reasonable degree of certainty.
Viral infections
Viral pathogens cause salivary gland infections more often than bacteria. The parotid gland is more susceptible compared to the submandibular gland as the salivary secretion is more serous. Serous saliva lacks lysosomes, IgA, and glycoproteins, which have anti-infective properties. These infections occur when pathogens enter the gland through the salivary duct. Reduction in the salivary flow, caused by dehydration, medications, radiation, and Sjögren’s syndrome, are predisposing factors. Table 8.1 lists the viral pathogens that can cause salivary gland infections.
Table 8.1 Viral causes of parotitis | |||||||
|---|---|---|---|---|---|---|---|
|
MUMPS
Mumps caused by paramyxovirus is the most common viral infection, usually involving the parotid gland. This is a RNA virus transmitted by airborne droplets. After an incubation period of 2-3 weeks, low-grade fever, malaise, and anorexia occur. This is then followed by parotitis, which is usually bilateral. Enlargement of the gland can be differentiated from cervical lymphadenopathy by outward displacement of the lobule of the pinna (8.1). Spontaneous resolution is the norm, but this can take a few weeks. Mumps can be associated with other serious complications such as sensorineural hearing loss, aseptic meningitis, orchitis, and pancreatitis. The clinical presentation should suggest the diagnosis. Serological tests to identify antibody to mumpsspecific IgM will confirm a recent infection. Treatment involves supportive care and recognizing the possible complications, which often need medical input. Use of the live attenuated MMR (mumps, measles, and rubella) vaccine has led to a decrease in the incidence of this disease.
 8.1 (A) Patient with mumps depicting parotid gland enlargement with cervical lympadenopathy. (B) The same patient after she fully recovered. |
HUMAN IMMUNODEFICIENCY VIRUS
Human immunodeficiency virus (HIV) causes a chronic infective process in the salivary glands. Enlargement of intra- or periparotid nodes and lymphatic infiltration of the glandular structure causes bilateral, noninflammatory, diffuse hypertrophy of the salivary glands (8.2). Lymphoepithelial cysts can also result from duct obstruction. The diagnosis is suspected from the clinical picture in persons known to be HIV positive. Rarely is the diagnosis made retrospectively from tissue biopsy from the salivary gland. Imaging (CT or MR scans) will differentiate parenchymal hypertrophy from lymphoepithelial cysts. The presence of multiple cysts may require a parotidectomy for cosmetic reasons. Parenchymal hypertrophy may settle with antiretroviral treatment.
Bacterial infections
ACUTE SUPPURATIVE SIALADENITIS
Acute suppurative sialadenitis is commonly seen in the postoperative setting following major surgery and in patients with chronic illnesses such as diabetes mellitus and renal failure. Calculus obstruction of the duct, more frequent in the submandibular salivary gland, can lead to secondary infection of the gland (8.3, 8.4). A similar syndrome of neonatal parotitis, often bilateral, is seen in pre-term neonates.
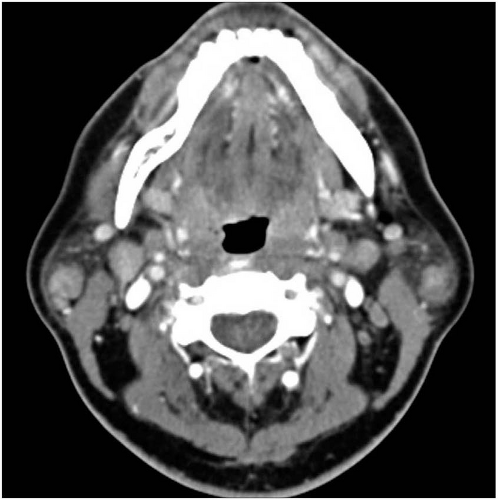 8.2 Bilateral intraparotid nodes causing parotid enlargement in HIV infection.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|