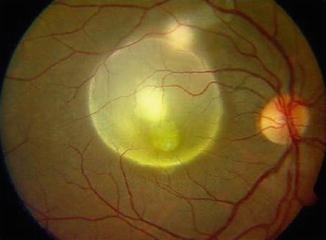
Fig. 12.1
(a) Fundus photograph shows an active focus of toxoplasmic retinochoroiditis adjacent to an old pigmented scar located at the superotemporal the superior vascular arcade in the vicinity of the optic disk. (b) Early-phase fluorescein angiogram shows hypofluorescence of both active and old focus. (c) Late-phase fluorescein angiogram shows peripheral hyperfluorescence and persistent central hypofluorescence of the active lesion with vascular leakage and optic disk hyperfluorescence. (d) Early-phase indocyanine green angiogram shows hypofluorescence of the retinochoroiditis focus. (e) Late-phase indocyanine green angiogram shows persistence of hypofluorescence of the retinochoroiditis focus with multiple satellite dark dots and retinal vascular staining. (f) Optical coherence tomography reveals a subclinical serous retinal detachment (arrow) with foveal involvement
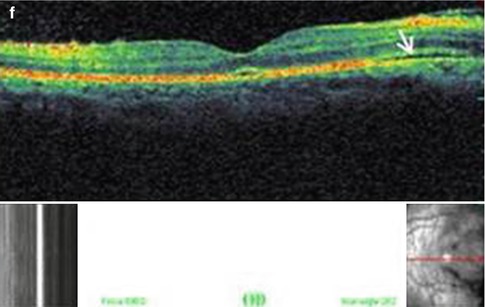
However, 25–35 % of eyes with active toxoplasmic RC do not exhibit associated old scar (Fig. 12.2). RC lesions may have various sizes and may occur in the posterior pole, sparing or involving the center, in periphery, or occasionally immediately adjacent to or directly involving the optic disk. Various associated fundus changes may occur including focal or diffuse retinal vein sheathing, retinal arterial involvement especially in the form of Kyrieleis arteriolitis, retinal hemorrhages, macular edema, serous retinal detachment (SRD), and optic disk hyperemia.
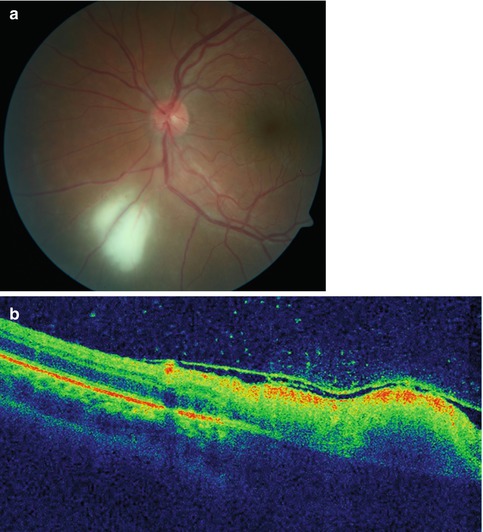
Fig. 12.2
(a) Fundus photograph shows an active focus of toxoplasmic retinochoroiditis without old scar. (b) Optical coherence tomography shows increased retinal reflectivity and thickening of the active lesion, retinal pigment epithelial and choriocapillaris band shadowing, posterior hyaloid thickening and detachment, and vitreous hyperreflective dots
The course of toxoplasmic RC is self-limiting in immunocompetent patients. The inflammation gradually resolves in 6–8 weeks, and a chorioretinal scar replaces the active lesion [7].
Ocular toxoplasmosis is a progressive and recurrent disease, with new lesions occurring at the margins of old scars as well as elsewhere in the fundus. Recurrences are totally unpredictable and may occur years after the original lesion resolved. Recurrence rates of 40–79 % have been reported [10].
The classic presentation of congenital toxoplasmosis is RC with a predilection for the posterior pole and macula (Fig. 12.3). Congenital toxoplasmosis may be bilateral in approximately 85 % of affected individuals [11–13] (Fig. 12.3).
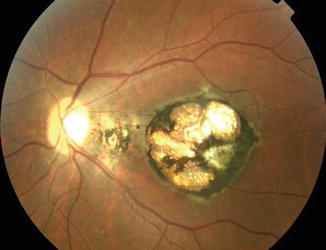
Fig. 12.3
Fundus photograph shows congenital toxoplasmosis involving the macula
RC developing in immunocompromised and older patients may present with atypical findings, including large, multiple, and/or bilateral lesions, with or without associated chorioretinal scars.
Other atypical presentations of toxoplasmic RC include punctate outer or inner retinal toxoplasmosis, neuroretinitis, optic neuritis, intraocular inflammation without RC, unilateral pigmentary retinopathy simulating retinitis pigmentosa, scleritis, and a presentation in association with Fuchs uveitis syndrome [14].
Early and late complications of ocular toxoplasmosis include retinal vascular occlusions (Fig. 12.4), SRD, choroidal ischemia, cataract, posterior synechiae, significant vitreous opacification and organization, rhegmatogenous or tractional retinal detachment, preretinal neovascularization, vitreous hemorrhage, choroidal neovascularization (CNV), epiretinal membrane (ERM), subretinal fibrosis, vasoproliferative tumor, optic atrophy, glaucoma, and phthisis bulbi [9, 10, 15].

Fig. 12.4
Color fundus photograph of the left eye of a patient with ocular toxoplasmosis shows an active focus of retinochorioretinitis adjacent to old pigmented scars infero-temporally and an area of retinal whitening along the inferior temporal arcade consistent with a diagnosis of branch retinal artery occlusion
12.1.1.4 Imaging
Fluorescein angiography (FA) shows early hypofluorescence of active focus of RC, followed by gradual staining starting from the lesion borders (Fig. 12.1). This imaging modality is useful in the detection and evaluation of associated retinochoroidal vascular changes including focal or diffuse retinal vascular leakage, macular edema, retinal or choroidal vascular occlusion, optic disk leakage, CNV, and retinochoroidal anastomosis [7, 8].
Indocyanine green angiography (ICGA) shows hypofluorescence of the main focus of RC at all phases of the angiogram (Fig. 12.1) [16]. ICGA also shows in up to 75 % of cases multiple hypofluorescent satellite dark dots, possibly due to choriocapillaris hypoperfusion, that disappear after therapy in the majority of cases (Fig. 12.1). More pronounced choroidal ischemia could be confirmed by ICGA in a subset of patients of patients with toxoplasmic RC [17, 18].
Optical coherence tomography (OCT) is a noninvasive test that is useful in evaluating and monitoring active toxoplasmic RC and associated changes. Findings include increased retinal reflectivity and thickening of the active lesion, retinal pigment epithelial and choriocapillaris band shadowing, posterior hyaloid thickening and detachment, vitreoschisis, vitreous hyperreflective dots, ERM, and SRD (Figs. 12.1 and 12.2). Disorganization of the retinal layers reflectivity with interruption of the inner/outer segment (IS/OS) junction due to scar formation may be observed [18–22]. Imaging of congenital toxoplasmosis macular scars reveals retinal thinning, retinal pigment epithelial hyper-reflectivity, excavation, intraretinal cysts, and fibrosis [23].
Ultrasonography is useful when view of the fundus is limited by posterior synechiae or vitreous opacity. The most frequent findings include intravitreal opacities, thickening of posterior hyaloids, partial or complete posterior vitreous detachment, focal retinochoroidal thickening, and tractional and rhegmatogenous retinal detachment.
12.1.1.5 Laboratory Investigations
The diagnosis of toxoplasmic RC is primarily based on typical clinical findings, but laboratory testing may be required to confirm the diagnosis in atypical clinical presentations. A positive serological assay for IgG does not confirm the diagnosis of ocular toxoplasmosis, given the high rate of seropositivity in the normal population in most countries. The presence of IgM and/or IgA titer or a rising IgG titer indicates recent acquired infection. A negative serology can exclude the diagnosis of ocular toxoplasmosis [25].
The Goldmann-Witmer (GW) coefficient and the western blot technique are used to demonstrate local production of antibodies in aqueous humor or rarely in vitreous fluid. A GW coefficient of greater than three is considered highly suggestive of a diagnosis of active ocular toxoplasmic infection [26].
12.1.1.6 Differential Diagnosis
Typical toxoplasmic RC can be easily differentiated for other infectious or noninfectious uveitic entities. Atypical clinical presentations should be differentiated from other infectious diseases, including necrotizing viral retinitis, tuberculosis, syphilis, bartonellosis, rickettsiosis, Lyme disease, fungal retinitis, bacterial retinitis, and toxocariasis [7, 8].
Toxoplasmic RC should also be differentiated from noninfectious entities including multifocal choroiditis, acute posterior multifocal placoid pigment epitheliopathy (APMPPE), serpiginous choroiditis, punctate inner choroidopathy, sarcoidosis, Behçet disease, ocular lymphoma, and other causes of optic nerve involvement [29].
Differential diagnosis of congenital ocular toxoplasmosis in newborns and young children mainly includes Rubella, CMV, Herpes, Syphilis, Toxocariasis, West Nile virus fever, acute lymphocytic choriomeningitis, macular coloboma, persistent hyperplastic vitreous, and neoplastic entities such as retinoblastoma and retinocytoma [29].
12.1.1.7 Treatment
Treatment of ocular toxoplasmosis remains controversial. However, the generally accepted criteria for treatment include the following: involvement of zone 1, especially in patients with active lesion affecting or threatening the fovea or optic nerve, lesion size >2 disk diameters, marked vitritis, retinal vascular occlusion, immunocompromised patients, elderly patients, and acquired toxoplasmosis [8, 9].
Some clinicians may elect to observe small lesions in the retinal periphery that are not associated with a significant decrease in vision or vitritis, while others treat virtually all patients in an effort to reduce the number of subsequent recurrences [9].
Numerous agents have been used to treat toxoplasmosis over the years [30, 31]. The standard treatment of ocular toxoplasmosis includes a combination of pyrimethamine, given in a loading dose of 100 mg on day 1 followed by 50 mg daily (25 mg in children), sulfadiazine 4 g/day, and corticosteroids (0.5–1 mg/Kg/day, depending on the severity of the inflammation). Folinic acid (25 mg per os two or three times a week) is added to prevent bone marrow suppression that may result from pyrimethamine therapy [30, 32, 33].
Corticosteroids should be used orally, always under anti-toxoplasmic therapy and begun within 48 h. The use of periocular or intravitreal corticosteroids should be avoided. Corticosteroids should also be avoided in immunocompromised patients. In general, treatment lasts from 4 to 6 weeks, at which time inflammation begins to subside and the retinal lesion shows signs of consolidation. This period may be extended if there is persistent disease activity.
Other alternatives include oral clindamycin, spiramycin, and azithromycin [9, 30]. The combination of pyrimethamine and azithromycin (500 mg on day 1, followed by 250 mg/day) is as effective, but less toxic, than the classic combination of pyrimethamine and sulfadiazine [8, 34].
Intravitreal clindamycin injection to treat toxoplasmosis RC is a promising approach [35].
Newborns with congenital toxoplasmosis are commonly treated with pyrimethamine and sulfonamides for 1 year, in consultation with a pediatric specialist. In cases of newly acquired toxoplasmosis during pregnancy, spiramycin 400 mg three times daily may be used [36].
Pyrimethamine should be avoided or used in lower dosage for the management of ocular toxoplasmosis in patients with HIV/AIDS who receive highly active antiretroviral therapy. Atovaquone is an alternative in these patients [37].
Vitreoretinal surgery will be required for vitreous opacities and for tractional or rhegmatogenous retinal detachment.
CNV can nowadays be successfully treated with intravitreal injection of anti-vascular endothelial growth factor (VEGF) [38, 39].
Prevention of toxoplasmosis mainly consists of measures to avoid exposure to infectious agent. Long-term intermittent use of one tablet of trimethoprim (160 mg)/sulfamethoxazole (800 mg) every 3 days was shown to decrease the risk of reactivation among patients with recurrent toxoplasmic RC [40].
12.1.2 Toxocariasis
Toxocariasis is a zoonotic disease caused by the infestation of humans by second-stage larvae of the dog nematode Toxocara canis or the cat nematode Toxocara cati. Toxocariasis manifests itself in one of two disease states: visceral larva migrans, the systemic form of the disease, or ocular larva migrans, the ocular form. It is rare for ocular toxocariasis (OT) to coexist with visceral larva migrans.
12.1.2.1 Epidemiology
OT is a worldwide distributed infection. It is an uncommon disease, with a prevalence ranging between 0 and 3.1 % of all uveitis cases [41, 42]. OT is predominantly a unilateral condition that occurs primarily in childhood but also can affect adults. The median patient age was found to be 11.5 years (range, 1–66 years) [43]. OT affects females and males with approximately equal frequency.
12.1.2.2 Life Cycle and Pathogenesis
The definitive hosts of Toxocara are dogs and cats. When infected, these animals pass Toxocara eggs in their feces into the environment. Once in the environment, it takes 2–4 weeks for Toxocara larva to develop in the eggs and for the eggs to become infectious. In dogs and cats, the life cycle is completed when the eggs are ingested and the larvae develop into adult worms in the intestine. Humans and other animals become infected through the unintentional ingestion of infectious eggs, which are found in soil contaminated by dog and cat feces. Infection rarely may occur when a person ingests undercooked meat from an animal infected with the Toxocara parasite. Children who have close contact with dogs, especially puppies, are at high risk for infection.
Ocular disease is caused by the migration of Toxocara larva through blood vessels in the circulatory system into the posterior segment of the eye [42]. Tissue damage is due to the host inflammatory reaction more than the infection itself.
12.1.2.3 Clinical Features
Patients present with unilateral decreased vision that may be accompanied by pain, photophobia, floaters, strabismus, or leukocoria. The anterior segment is typically quiet. However, nongranulomatous anterior inflammation and posterior synechiae may be present with severe disease. Posterior segment findings include three recognizable ocular syndromes: peripheral granuloma, posterior pole granuloma, and chronic endophthalmitis [41].
Peripheral granuloma is the most common clinical presentation of OT, occurring in nearly half of patients. It usually appears as a focal, elevated, white peripheral nodule, surrounded by pigmentary changes and associated with traction vitreoretinal bands that may extend from the peripheral mass to the optic nerve head (Fig. 12.5).
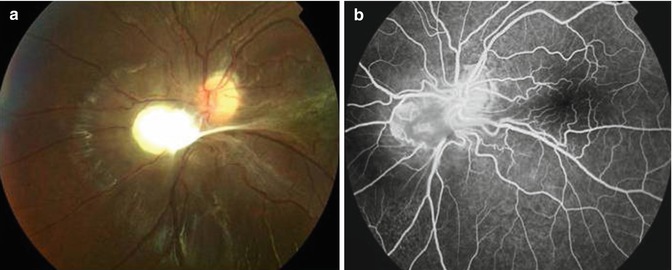
Fig. 12.5
(a) Fundus photograph shows a toxocara granuloma adjacent to the optic disk inferonasally with associated vitreoretinal traction (b) Late-phase fluorescein angiogram shows heterogeneous hyperfluorescence of the granuloma and associated retinal vascular tortuosity
Posterior pole involvement is observed in one quarter of cases. The retinochoroidal granuloma may vary in size from less than one to two disk diameters and may spare or involve the fovea [41].
OT presents in nearly one quarter of patients in the form of chronic endophthalmitis with anterior uveitis and diffuse vitritis with a poor view of the fundus. Hypopion and retinal detachment may occur in severe cases [43–47]. Other less common clinical presentations of OT are optic neuritis, neuroretinitis, and mobile living larva in the eye [46].
Complications of OT include macular heterotropia, amblyopia, cataract, secondary glaucoma, ERM, retinal folds and tractional retinal detachment, macular scar from macular granuloma, cystoid macular edema (CME), detachment of the ciliary body and anterior choroid with hypotony, neovascular membranes, and phthisis bulbi. Visual loss is commonly caused by inflammation of the vitreous and traction retinal detachment [41, 43].
12.1.2.4 Imaging
On FA, the granuloma is characterized by central hyperfluorescence with early-phase dye leakage (Fig. 12.5). Diffuse ischemic area in the periphery has also been reported [48].
The most characteristic ultrasonographic findings include highly reflective peripheral mass, pseudocystic transformation of the peripheral vitreous, vitreous membranes or retinal fold extending from the mass to the posterior pole, and tractional retinal detachment [49].
Ultrasound biomicroscopy (UBM) may be also useful in patients with opaque media or hypotony by showing pseudocystic transformation of the peripheral vitreous, a highly sensitive, but not specific, finding [50, 51].
On OCT, posterior pole granuloma may appear as a highly reflective mass protruding above the retinal pigment epithelium (RPE) [52, 53]. OCT may also show most important vitreoretinal tractions on macular region and optic disk and subretinal fluid.
Computed tomography (CT) and magnetic resonance imaging (MRI) are helpful for the differential diagnosis with retinoblastoma [46].
12.1.2.5 Laboratory and Ancillary Tests
ELISA testing has a high sensitivity and specificity in patients with a presumptive diagnosis of OT [43]. Current serologic testing for antibody to the Toxocara parasite does not reliably indicate active infection. In fact, studies have shown that the immunoglobulin-G Toxocara antibody can remain detectable for years after treatment, which limits the applicability of the test to monitor treatment success [54]. GW coefficient analysis in aqueous humor or vitreous may help establish the diagnosis of OT [55].
12.1.2.6 Differential Diagnosis
The most important differential diagnosis of OT consideration is retinoblastoma. Other entities to consider include infectious endophthalmitis, toxoplasmosis, pars planitis, sarcoidosis, syphilis, and congenital retinovascular abnormalities such as retinopathy of prematurity, persistent fetal vasculature, Coats disease, and familial exudative vitreoretinopathy.
12.1.2.7 Treatment
Although there is no uniformly satisfactory treatment for OT, medical therapy with periocular and systemic corticosteroids continue to be the therapeutic mainstay for eyes with active vitritis to reduce the inflammatory response to prevent structural complications [46, 47]. The utility of antihelminthic therapy such as albendazole, thiabendazole, or mebendazole is still controversial. Vitreoretinal surgery has been successfully used to manage complications such as rhegmatogenous and tractional retinal detachments, ERM, and persistent vitreous opacification [56]. Prognosis depends on the age of presentation, location of toxocara lesion, and subsequent complications.
12.1.3 Diffuse Unilateral Subacute Neuroretinitis (DUSN)
Diffuse unilateral subacute neuroretinitis (DUSN), first described by Gass et al. in 1978 [57], is an infectious ocular disease caused by an unidentified motile nematode capable of infiltrating the subretinal space, causing inflammation and retinal degeneration that lead to profound vision loss [58].
12.1.3.1 Pathogenesis
Evidence to date suggests that DUSN is caused by solitary nematodes of two different sizes that migrate through the subretinal space. The smaller worm, measuring 400–1.000 μm in length, has been proposed to be either Ancylostoma caninum (the dog hookworm) or Toxocara canis, the latter being endemic to the southeastern United States, Caribbean islands, and Brazil. The larger worm is believed to be Baylisascaris procyonis (the raccoon roundworm), which measures 1.500–2.000 μm in length and has been found in the northern Midwestern United States and Canada [44, 46]. DUSN appears to involve an inflammatory or a local toxic tissue effect on the outer retina caused by the worm by-products left behind, as well as a more diffuse toxic reaction affecting both the inner and outer retina.
12.1.3.2 Epidemiology
Initially described in the Southeastern and Midwestern parts of the United States and the Caribbean islands, DUSN has also been reported in other parts of North America, in South America, in Northwestern Europe, China, and Africa [44, 46, 59, 60]. In Brazil, DUSN is considered an important cause of posterior uveitis in children and young healthy adults. The disease can affect children and young adults without gender preference or systemic problems. It is usually unilateral and occasionally is bilateral.
12.1.3.3 Clinical Features
The onset of DUSN is usually insidious. Some patients in the early stages of the disease complain of unilateral paracentral or central scotoma, ocular discomfort, or transient obscurations of vision [61]. Patients are usually in good general health. Clinical findings in patients with DUSN can be divided into two stages. The early stage is characterized by mild to moderate vitritis, mild optic disk edema, and recurrent crops of evanescent, multifocal, yellow-white lesions at the level of the outer retina and choroid with continued visual loss and central scotoma (Fig. 12.6). The white lesions are clustered within a small zone and fade over a few weeks leaving pigment mottling. Focal retinal hemorrhages and perivenous exudation may be rarely seen. Careful observation in the vicinity of the white lesions may show a small white nematode. Occasionally, a few patients may demonstrate mild anterior uveitis with cells, flare, and keratic precipitates. The late stage of the disease is characterized by optic disk atrophy, retinal vessel narrowing, and focal or diffuse RPE degeneration marked by profound visual loss. The worm can be identified at any stage of the disease [45].
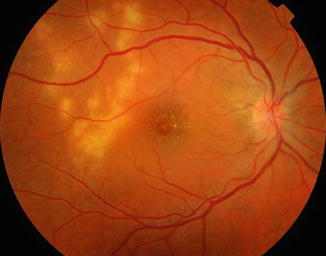
Fig. 12.6
Fundus photograph of a patient with DUSN shows a cluster of gray-white lesions (Courtesy, Carlos Pavesio)
12.1.3.4 Imaging
FA usually demonstrates mild leakage of dye from the capillaries on the optic disk and some of the retinal vessels. The gray-white lesions are nonfluorescent or hypofluorescent early and stain in the late phase of the angiogram.
ICGA may reveal hypofluorescent dark spots, and hyperfluorescence at the macular level [62]. ICGA could be a useful tool for the detection of subretinal nematodes [63].
Spectral domain OCT showed that RNFL and central retinal thickness were thinner in DUSN eyes compared to normal eyes. Late-stage disease had more pronounced thinning compared to early-stage patients. This thinning in retinal nerve fiber layer (RNFL) and central retinal thickness may reflect the low visual acuity in patients with DUSN [64].
Electroretinography in the affected eye is usually reduced quite early in the course of the disease and is more severely reduced with the b-wave being affected more than the a-wave in the later stage of the disease [44, 46]. Goldman perimetry is useful to evaluate remaining visual field before and after treatment of the disease.
12.1.3.5 Differential Diagnosis
Early signs of DUSN often are mistaken for multifocal choroiditis, sarcoidosis, acute posterior multifocal placoid pigment epitheliopathy, multiple evanescent white dot syndrome, serpiginous choroiditis, Behçet disease, ocular toxoplasmosis, nonspecific optic neuritis, and papillitis. Late features of the disease may be confused with posttraumatic chorioretinopathy, occlusive vascular disease, toxic retinopathy, unilateral optic atrophy, and retinitis pigmentosa [61].
12.1.3.6 Treatment
Therapy is limited in patients with DUSN. If the worm is visualized, laser treatment of the nematode with confluent laser burns 100–200 μ in size can be highly effective and may improve visual acuity and inflammatory ocular signs [46]. The worm can be induced to migrate away from the macula before treatment by directing a bright light on it. The worm may also be surgically removed for identification purposes. Chemotherapy with anthelmintic drugs, such as mebendazole, thiabendazole, or albendazole may be the only treatment available when a worm cannot be visualized, but success is often difficult to document. A treatment regimen of albendazole 400 mg daily for 4 weeks seems to be safe and beneficial for patients with DUSN [65].
Treatment with corticosteroids has shown transient suppression of the inflammation without altering the final outcome of the disease. Patients with retinal complications caused by the inflammation may benefit from surgical intervention in some cases.
12.2 Other Parasitic Diseases
12.2.1 Onchocerciasis
Onchocerciasis, also named river blindness or Robles disease, is a parasitic disease caused by the microfilariae Onchocerca volvulus [45]. O. volvulus is transmitted by the bite of the black Simulium fly, which breeds in rapidly flowing waters. The clinical manifestations of onchocerciasis range from no skin or eye lesions to very severe skin involvement and blindness.
12.2.1.1 Epidemiology
Onchocerciasis is endemic in many areas of sub-Saharan Africa and in isolated foci in Central and South America. It is rarely seen or diagnosed in the Western world. According to the World Health Organization, at least 18 million people are infected, of whom almost 300.000 are blind [66]. In hyperendemic areas, every one over the age of 15 is infected, and half will become blind before they die.
12.2.1.2 Pathogenesis
Humans are the only host for O. volvulus. The O. volvulus larvae are transmitted through the bite of female black flies of the Simulium genus. The larvae develop into mature adult worms that form subcutaneous nodules. The adult female releases millions of microfilariae that migrate throughout the body, particularly to the skin and the eye.
The ocular manifestations of onchocerciasis are caused by the presence of dead parasites within the eye. The microfilariae penetrate the eye by the bulbar conjunctiva at the limbus and then invade the cornea, aqueous humor, and iris. They reach the posterior segment by the circulation or ciliary nerves, which supply the peripheral retina and choroid [46].
12.2.1.3 Clinical Features
Anterior segment involvement includes punctate keratitis, corneal opacity that turns to scar tissue, producing sclerosing keratitis in late stages [46]. An iridocyclitis also can be seen with atrophy of the iris, cataract, and glaucoma. Chorioretinal changes are also common. They typically begin in the periphery and vary widely in severity. Early disruption of the RPE is typical with pigment dispersion and focal areas of atrophy (Fig. 12.7). Later, severe chorioretinal atrophy occurs predominantly in the posterior pole with sheathing of the retinal vessels and visual field constriction. Optic disk atrophy is common in advanced disease. Macular edema can also be found.
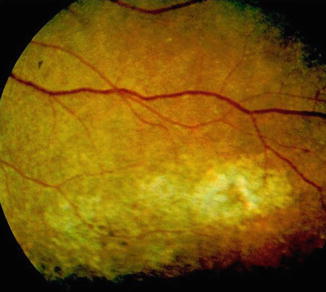
Fig. 12.7
Fundus photograph of a patient with onchocerciasis shows peripheral chorioretinal changes with pigment dispersion, and focal areas of atrophy (Courtesy, Aniki Rothova)
12.2.1.4 Laboratory Investigations
Diagnosis of onchocerciasis is made by extraction of microfilariae or adult worms from skin or subcutaneous nodules by biopsy or by identification of live microfilariae in the aqueous humor [67].
12.2.1.5 Treatment
Ivermectin, given in a single oral dose of 150 μg/kg, is the first choice to treat onchocerciasis. Annual ivermectin therapy seems to improve intraocular inflammation [67]. Topical corticosteroids can be used to control any anterior uveitis. Vector control strategies tend to have limited success.
12.2.2 Cysticercosis
Cysticercosis is a systemic illness caused by the Cysticercus cellulosae larvae of the adult tapeworm Taenia solium and Taenia saginata. The most frequently reported locations are skin, skeletal muscle, heart, eye, and most importantly, the central nervous system.
12.2.2.1 Epidemiology
Cysticercosis is a common cause of ocular inflammation in some developing countries such as Central and South America, India, Southeast Asia, China, Eastern Europe, and certain parts of Africa [45, 68]. Ocular cysticercosis is a disorder of the young, occurring most frequently between the ages of 10 and 30 years, without gender predilection.
12.2.2.2 Pathogenesis
Human infection is caused by Cysticercus cellulosae, the larval stage of the cestode Taenia solium. Human cysticercosis is caused by ingestion of water or foods contaminated by the pork tapeworm. The eggs mature into larvae, penetrate the intestinal mucosa, and spread hematogenously to the eye via the posterior ciliary arteries into the subretinal space in the posterior pole [46].
12.2.2.3 Clinical Features
Although cysticercosis may involve any structure of the eye and its adnexae, the posterior segment is most often involved. Depending on the location of the intraocular cyst, patients may present asymptomatically with relatively good vision or may complain of floaters, moving sensations, ocular pain, photophobia, redness, and very poor visual acuity. Larvae within the subretinal space may cause an exudative retinal detachment or may perforate the retina, causing a retinal break that may be self-limiting or associated with retinal detachment and gain access to the vitreous cavity. The characteristic clinical appearance is that of a globular or spherical translucent white cyst (Fig. 12.8), with a head or scolex that undulates in response to the examining light within the vitreous or subretinal space [45]. The cyst itself varies in size from 1.5 to 6 disk diameters. RPE atrophy may be observed surrounding the presumptive entry site of the cysticercus into the subretinal space [46]. Larvae death produces a severe inflammatory reaction characterized by zonal granulomatous inflammation surrounding necrotic larvae on histologic examination.