Fig. 9.1
Slit-lamp biomicroscopy of a 42-year-old woman with strongly positive tuberculin skin test (24 mm induration) shows mutton-fat keratic precipitates and posterior synechiae
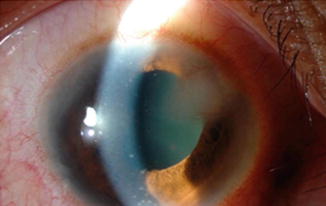
Fig. 9.2
Slit-lamp biomicroscopy of a 24-year-old woman with strongly positive tuberculin skin test (28 mm induration) shows interstitial keratitis and mutton-fat keratic precipitates
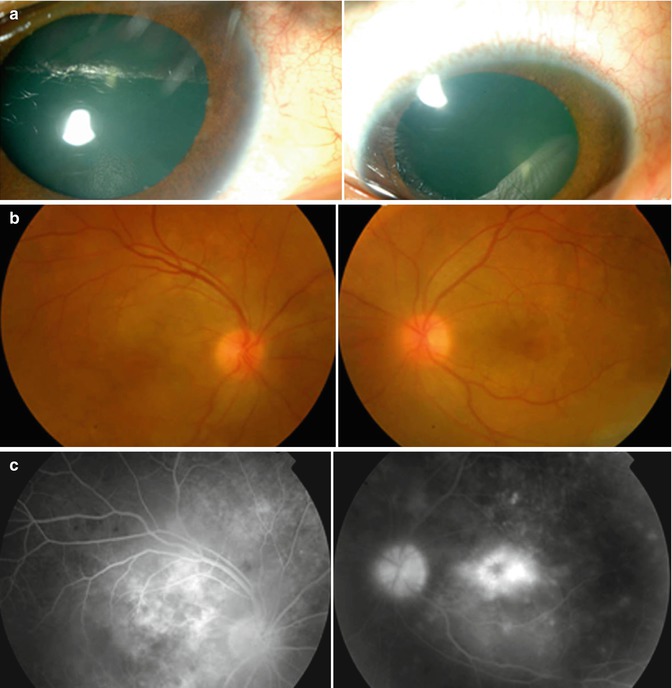
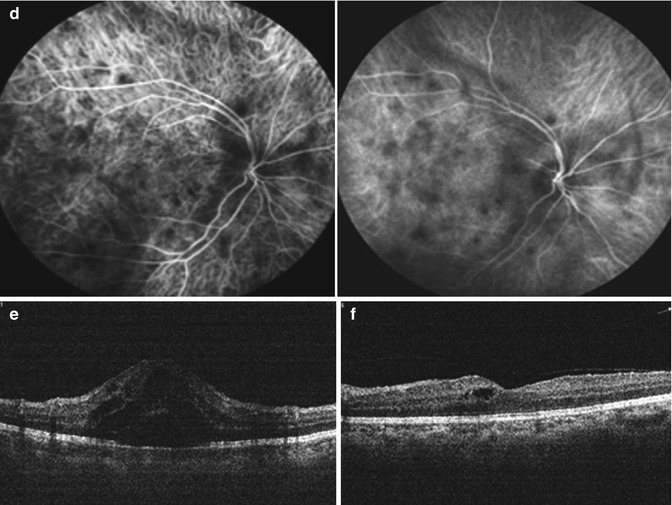
Fig. 9.3
A 32-year-old man with strongly positive tuberculin skin test (24 mm induration). Slit-lamp biomicroscopy shows bilateral iris nodules (a). Fundus photographs show disk swelling and hyperemia (b). Fluorescein angiography shows leakage from the optic nerve head and retinal vessels and cystoid macular edema (c). Indocyanine green angiography shows choroidal hypofluorescent areas (d). Optical coherence tomography shows cystoid macular edema. Visual acuity was 20/100 (e). Two months after starting antituberculous therapy and systemic corticosteroids, optical coherence tomography displays reduction of macular edema. Visual acuity improved to 20/30 (f)
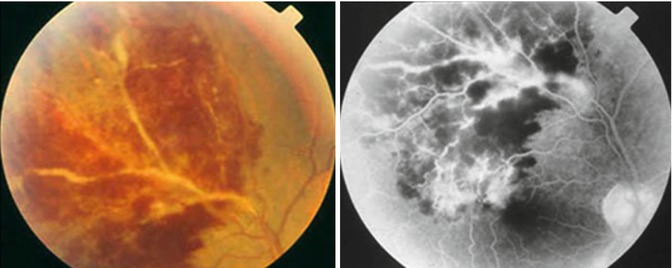
Fig. 9.4
Right eye of a 29-year-old man with strongly positive tuberculin skin test (24 mm induration) shows thick perivenous sheathing with intraretinal hemorrhage (left). Fluorescein angiography shows leakage from the retinal veins (right)
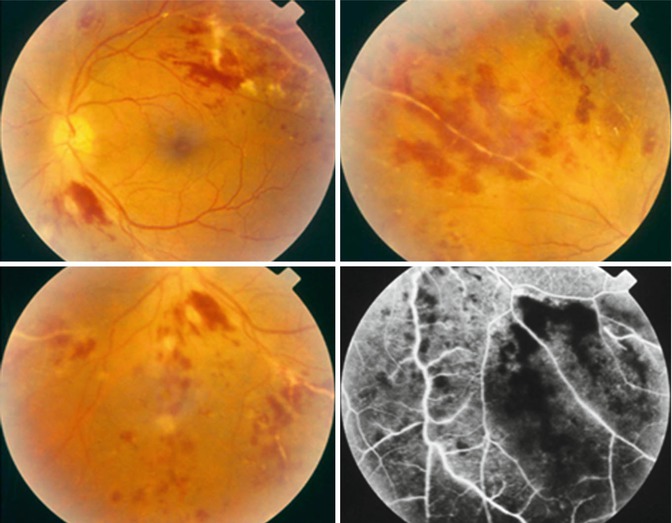
Fig. 9.5
Left eye of a 27-year-old man with strongly positive tuberculin skin test (16 mm induration) shows thick perivenous sheathing and intraretinal hemorrhages. Fluorescein angiography shows leakage from the retinal veins and retinal nonperfusion (bottom left)
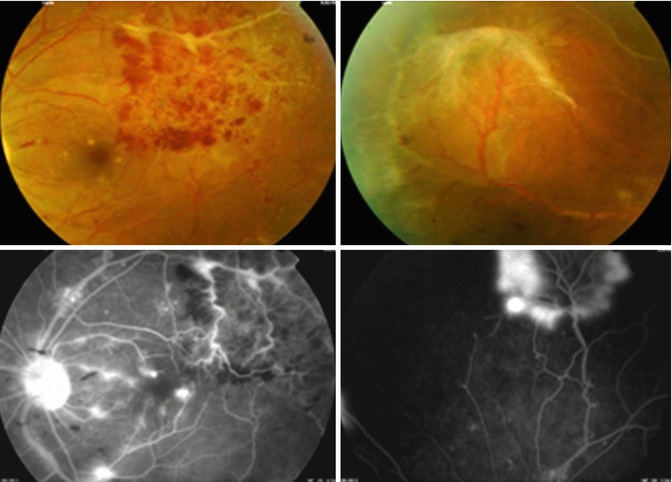
Fig. 9.6
Left eye of a 22-year-old man with strongly positive tuberculin skin test (22 mm induration) shows perivenous sheathing and intraretinal hemorrhages (top left) and peripheral sclerosed vessels and fibrovascular proliferation (top right). Fluorescein angiography shows leakage from the retinal vessels (bottom left), peripheral retinal nonperfusion, and leakage from the peripheral neovessels (bottom right)
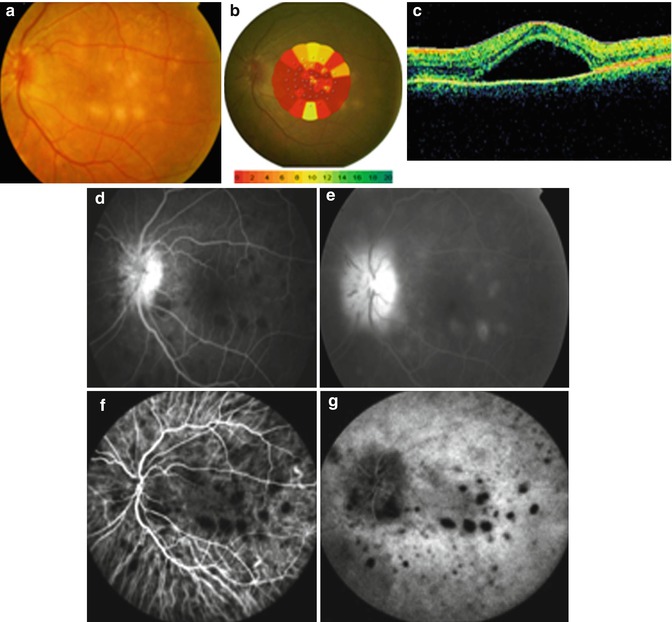

Fig. 9.7
Left eye of a 50-year-old woman with strongly positive tuberculin skin test (26 mm induration) shows multifocal choroiditis and disk swelling and hyperemia. Visual acuity was 20/100 (a). MP-1 microperimetry shows reduced sensitivity. The mean central retinal sensitivity was 1.1 decibels (dB). Color-coded, numeric scale shows the threshold in 2 dB steps from 0 to 20 dB. Normal sensitivity is indicated by green color and decreased sensitivity is indicated by red color (b). Optical coherence tomography shows exudative retinal detachment (c). On fluorescein angiography, the lesions are hypofluorescent in the early phase (d) and hyperfluorescent in the late phase (e). The optic nerve head shows leakage and staining. Indocyanine green angiography shows that the lesions are hypofluorescent throughout (f, g). Note that the lesions on indocyanine green angiography are more numerous than on fluorescein angiography. Six months after starting antituberculous therapy and systemic corticosteroids, visual acuity improved to 20/30. Fundus photography shows resolution of the lesions (h). The mean central retinal sensitivity improved to 11.1 dB (i). Optical coherence tomography displays resolution of exudative retinal detachment (j)
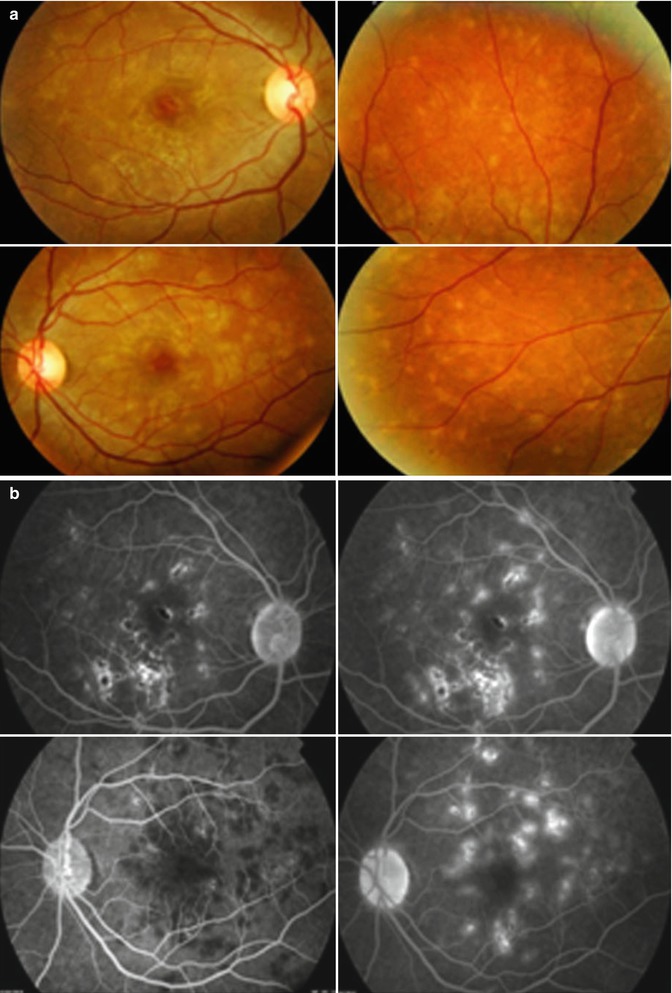
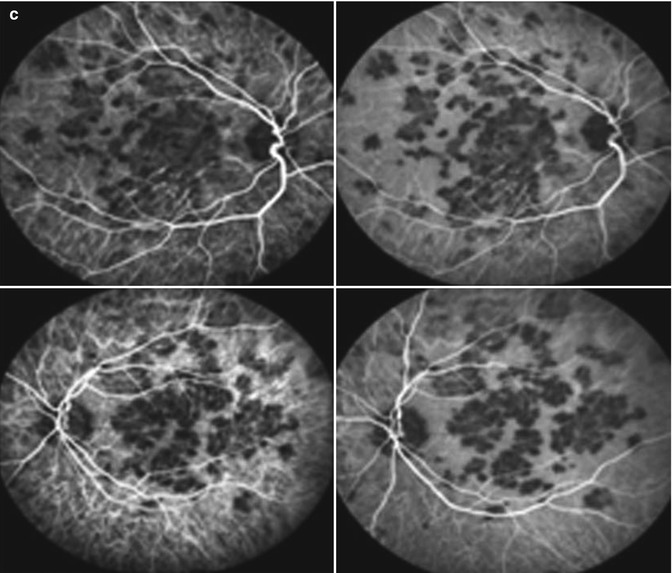
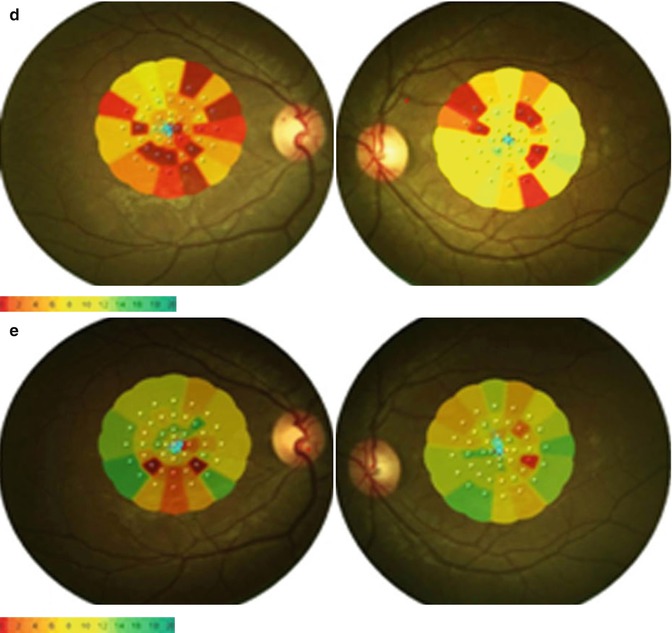
Fig. 9.8
A 30-year-old woman with strongly positive tuberculin skin test (30 mm induration). Fundus photographs show multifocal choroiditis. Visual acuity was 20/80 in the right eye and 20/30 in the left eye (a). Fluorescein angiography shows that the lesions are hypofluorescent in the early phase and hyperfluorescent in the late phase (b). Indocyanine green angiography shows that the lesions are hypofluorescent throughout (c). Note that the lesions on indocyanine green angiography are more numerous than on fluorescein angiography. At presentation, the mean central retinal sensitivity was 3.5 dB in the right eye and 8.0 dB in the left eye (d). Two months after starting antituberculous therapy and systemic corticosteroids, the mean central retinal sensitivity improved to 7.3 dB in the right eye and 13 dB in the left eye. Visual acuity improved to 20/20 in both eyes (e)
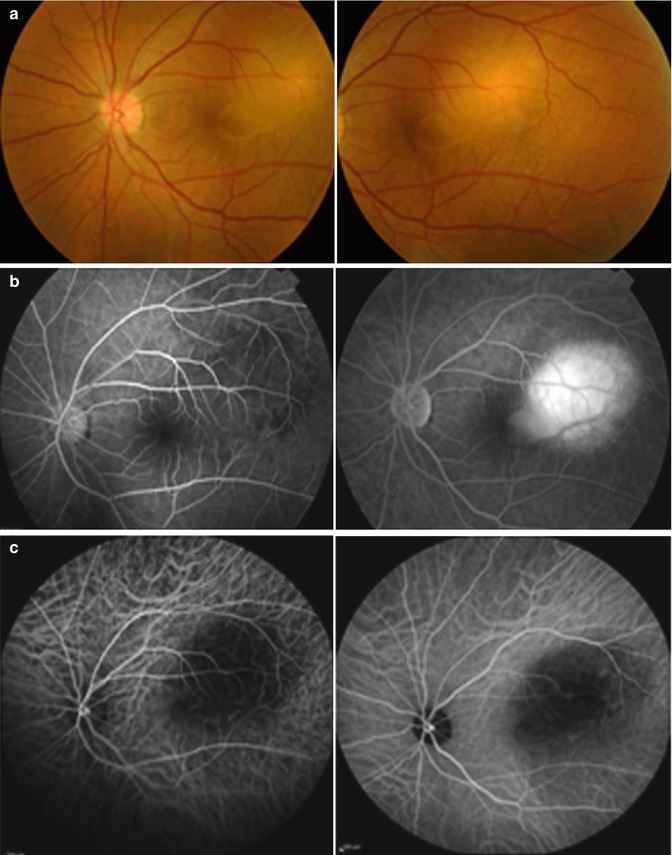

Fig. 9.9
Left eye of a 37-year-old man with strongly positive tuberculin skin test (18 mm induration). Visual acuity was measured by counting fingers at 3 ft. Fundus photographs shows subretinal amelanotic choroidal mass with exudative retinal detachment (a). Fluorescein angiography shows that the lesion is hypofluorescent in the early phase and hyperfluorescent in the late phase (b). Indocyanine green angiography shows that the lesion is hypofluorescent throughout (c). Optical coherence tomography shows exudative retinal detachment (d). Ultrasonography shows a solid elevated mass lesion on B-scan and a low internal reflectivity on A-scan (e). Two months after starting antituberculous therapy and systemic corticosteroids. Visual acuity improved to 20/25. Fundus photography shows resolution of the granuloma and chorioretinal scar. Optical coherence tomography displays resolution of exudative retinal detachment (f)

Fig. 9.10
Left eye of the a 45-year-old man with strongly positive tuberculin skin test (25 mm induration) shows widespread serpiginous-like areas of hyperpigmentary and hypopigmentary changes, which extended from the peripapillary region to mid-peripheral retina. Note the presence of active lesions in the macular area (arrow)
Choroidal tubercles and tuberculomas (large, solitary masses) are reported to be the most common intraocular manifestations of TB. The presence of choroidal tubercles is indicative of hematogenous seeding of bacilli [27]. There may be an overlying exudative retinal detachment. The differential diagnosis includes sarcoid granulomas, syphilitic gummas, and metastatic tumors. Choroidal TB might also present as multifocal progressive choroiditis, which shows progression to confluent, diffuse choroiditis with an active edge or diffuse choroiditis with amoeboid pattern and a leading edge. These morphologic presentations resemble serpiginous choroiditis [34, 38, 45].
Tuberculous retinal vasculitis is typically an obliterative periphlebitis affecting the retina in multiple quadrants, starting at or anterior to the equator and progressing posteriorly. Occasionally, it can begin close to the optic nerve head, mimicking a vein occlusion. Ophthalmoscopic findings vary and depend on the stage of the disease. Initially, it presents as active retinal periphlebitis with thick exudates around the retinal veins associated with retinal hemorrhages and hemorrhagic infarction of the retina. Active retinal periphlebitis is associated with mild degree of cellular infiltrate in the anterior chamber and mild vitreous infiltrate. Healed periphlebitis results in sclerosed venules and abnormal vascular anastomosis. The periphlebitis may cause nonperfusion of a substantial portion of the retina that may lead to proliferative vascular retinopathy with sequelae such as recurrent vitreous hemorrhage, traction retinal detachment, rubeosis iridis, and neovascular glaucoma [26, 31, 36]. Several studies reported that clinical signs significantly associated with presumed tuberculous uveitis include extensive posterior synechiae, retinal vasculitis with or without choroiditis, severe vitritis, and serpiginous-like choroiditis [46, 47]. Of these various intraocular changes, the most common clinical presentation appears to be panuveitis and posterior uveitis [43].
9.3 Diagnosis
In recent years, ocular involvement due to TB has reemerged associated with an increasing prevalence of TB. A high index of clinical suspicion is essential for the early diagnosis of tuberculous uveitis. Late diagnosis and delay in management can result in loss of the eye and can even be life threatening in severe conditions. The diagnosis should be considered by the ophthalmologist when unexplained chronic uveitis with the characteristic clinical signs occur that promptly recurs upon tapering corticosteroid and/or immunosuppressive therapy. Tuberculous retinal vasculitis should be suspected in the presence of florid retinal periphlebitis with marked capillary closure with a relatively mild degree of vitreous cellular infiltrate, particularly in patients of Asiatic origin: genetic predisposition may account for the propensity to develop retinal vasculitis in these patients [26]. Most patients with ocular involvement have no history of pulmonary or other systemic forms [26, 27, 35, 40, 43], making a definitive diagnosis difficult. Therefore, tuberculous uveitis is frequently misdiagnosed, and the disease is recognizable after a very long diagnostic delay [40].The absence of clinically evident pulmonary TB does not rule out the possibility of ocular TB, as about 60 % of patients with extrapulmonary TB have no evidence of pulmonary TB [48].
The diagnosis of ocular involvement with TB is considered in the setting of (1) isolation of M. tuberculosis from ocular fluid or tissue specimen by a microbiologic or histopathologic study. However, the process is prolonged as it may take several weeks before culture results become available for starting specific therapy. Moreover, obtaining biopsy specimens from intraocular tissues for making a confirmatory histopathological diagnosis is difficult with potential morbidity associated with obtaining the biopsy material from the eye, (2) as presumed ocular disease suggestive of TB with proven active systemic disease, or (3) as presumed ocular disease without evidence of active systemic disease [26]. In the last two situations, the diagnosis of ocular TB remains largely presumptive. Because of the difficulty in obtaining microbiologic evidence, in nearly all reported cases, the diagnosis of intraocular TB was only presumptive [26, 29, 30, 32–37, 40, 42].
In most studies, the diagnostic criteria for presumed tuberculous uveitis were [26, 29, 30, 32–37, 40, 43]:
1.
Ocular findings consistent with possible intraocular TB with no other cause of uveitis suggested by history of symptoms or ancillary testing
2.
Strongly positive tuberculin skin test results (≥15 mm area of induration/necrosis)
3.
Response to antituberculous therapy with absence of recurrences
Tuberculin skin test remains a vital part of systemic workup for uveitis patients as it provides supportive information when clinical signs and symptoms suggest TB. The test is carried out by injecting 5 tuberculin units intradermally to raise a wheal of 6–10 mm in diameter. Any induration is measured after 48–72 h. An induration of less than 5 mm is considered a negative result. The specificity of the tuberculin skin test for M. tuberculosis increases with larger skin reactions (Fig. 9.11) and with a history of exposure to an active case of TB [27]. It is important to note that the effect of neonatal vaccination with bacilli Calmette-Guérin (BCG) on tuberculin skin test declines over the first 7 years of life. In addition, it was demonstrated that an induration greater than 14 mm is unlikely to be due to prior BCG vaccination [49].

Fig. 9.11
A 30-year-old woman with presumed tuberculous uveitis with strongly positive tuberculin skin test (32 mm induration)
Interferon (IFN)-γ release assays are considered highly specific for M. tuberculosis because they are not confounded by prior vaccination for TB. A recent study [50] raised concerns about the sensitivity of QuantiFERON-TB Gold assay (QuantiFERON-TB Gold In-Tube, Cellestis, Carnegie, Australia) for detection of latent TB infection. In addition, another study demonstrated that there was no statistically significant difference in specificity between QuantiFERON-TB Gold assay and tuberculin skin test and that QuantiFERON-TB Gold assay may be less sensitive than the tuberculin skin test using a 15-mm induration cutoff value [51]. Kurup et al. [52] reported no demonstrable advantage of QuantiFERON-TB Gold test over tuberculin skin test for detection of latent TB infection in patients with granulomatous uveitis. Recently, Ang et al. [53] demonstrated that QuantiFERON-TB Gold assay was not superior to tuberculin skin test in sensitivity as a screening test or first-line study in TB-related uveitis. Similarly, Babu et al. [54] showed that QuantiFERON-TB Gold test is not specific for intraocular TB. In addition, Gineys et al. [55] showed a significantly higher median QuantiFERON-TB Gold value in a group of tuberculous uveitis patients with a successful therapeutic response to full antituberculous treatment compared to the group with treatment failure. A recent study showed that TB history or contact in the past and associated retinal vasculitis were significantly associated with tuberculosis-related uveitis. Sensitivity and specificity of the tuberculin skin test and QuantiFERON-TB Gold assay did not differ significantly with fair agreement [56].
Polymerase chain reaction (PCR) is a molecular technique used to detect mycobacterial DNA in clinical specimens. The false-positive PCR results and the low specificity of PCR might challenge the understanding of PCR results [57]. Aqueous, vitreous, and epiretinal membranes from patients with presumed TB uveitis are used as specimens for PCR. However, sensitivity was reported to be low [33]. Enzyme-linked immunosorbent assay detection of IgG antibodies against purified cord factor prepared from M. tuberculosis may be useful to support the diagnosis of presumed tuberculous uveitis [30]. Chest computed tomography (CT) is more sensitive in detecting presence, dimensions, and activity of tuberculous mediastinal lymphadenopathy which routine chest x-rays cannot detect in patients with presumed TB uveitis [58]. Recently, it was demonstrated that the use of positron emission tomography/CT is useful to identify lesions appropriate for biopsy and helps to establish the diagnosis [59].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


