Fig. 10.1
(a) Red-free photograph of the left eye reveals an active, nonelevated, placoid, outer retinal lesion in the macula. (b) Late-phase fluorescein angiogram shows a geographic hyperfluorescent area and optic disk leakage (Courtesy, Bahram Bodaghi)
Patients with acute syphilitic posterior placoid chorioretinitis show characteristic outer retinal abnormalities on SD OCT imaging including disruption of the inner segment/outer segment band, nodular thickening of the RPE with loss of the linear outer segment/RPE junction, and, in some cases, loss of the external limiting membrane, accumulation of subretinal fluid, and punctate hyperreflectivity in the choroid [19, 20].
Syphilitic uveitis can also manifest as retinitis without choroidal involvement, involving the posterior pole or the periphery (Fig. 10.2). The retinitis may be associated with vasculitis, papillitis, and vitritis with minimal if any anterior segment inflammation [14]. In addition to vessel wall staining and vascular and optic nerve leakage, FA may reveal intraretinal lesions in the areas of retinitis. Punctate retinitis with inner retinal and preretinal white dots is a possible feature of ocular syphilis [12, 15, 21].
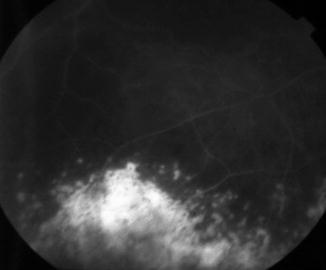
Fig. 10.2
Late-phase fluorescein angiogram shows multiple peripheral hyperfluorescent areas of retinitis. (Courtesy, Bahram Bodaghi)
Syphilis can present as a necrotizing retinitis in the midperiphery and peripheral retina and may resemble acute retinal necrosis or progressive outer retinal necrosis [22].
Isolated retinal vasculitis that affects the retinal arterioles, capillaries, and larger arteries or veins, or both, is another feature of syphilitic intraocular inflammation that may best be appreciated on FA. Focal retinal vasculitis may masquerade as a branch retinal vein occlusion.
Neuro-ophthalmic manifestations of syphilis include the Argyll Robertson pupil, ocular motor nerve palsies, isolated papillitis, optic neuropathy, neuroretinitis, and retrobulbar optic neuritis, which all appear most often in patients with tertiary syphilis or in neurosyphilis. Progressively visual loss secondary to optic atrophy can be seen as a manifestation of tertiary syphilis [6].
Ocular involvement in syphilis patients with HIV infection in the HAART era is more frequently bilateral and seems to involve the posterior segment more often with high frequencies of posterior uveitis, posterior placoid chorioretinitis, necrotizing retinitis, and optic nerve involvement [7, 10, 23–26].
10.2.2 Congenital Syphilis
Ocular inflammatory signs of syphilis may present at birth or decades later and include uveitis, interstitial keratitis, optic neuritis, glaucoma, and congenital cataract. A multifocal chorioretinitis and, less commonly, retinal vasculitis are the most frequent uveitic manifestations of early congenital infection [8]. Consequently, a bilateral “salt and pepper” fundus may develop, affecting the peripheral retina, posterior pole, or a single quadrant. These changes are not progressive, and the patient may have normal vision. A less commonly described funduscopic variation is that of a bilateral secondary degeneration of the RPE, which may mimic retinitis pigmentosa with narrowing of the retinal and choroidal vessels, optic disk pallor with sharp margins, and morphologically variable deposits of pigment [8].
10.3 Laboratory Investigations
The diagnosis of syphilitic uveitis is usually based on history and clinical presentation and is supported by a combination of Treponema-specific tests, such as the Venereal Disease Research Laboratory (VDRL) and rapid plasma reagin (RPR), and nontreponemal tests, such as the fluorescent treponemal antibody-absorption test (FTA-ABS) and T. pallidum particle agglutination test (TP-PA) [10].
False-positive nontreponemal and treponemal test results may be seen in case of systemic lupus erythematosus, leprosy, advanced age, intravenous drug abuse, bacterial endocarditis, tuberculosis, vaccinations, infectious mononucleosis, HIV infection, atypical pneumonia, malaria, pregnancy, rickettsial infections, and other spirochetal infections [10]. Subsequently, the use of only one serological test is insufficient in making the diagnosis. Patients should be initially tested using one of the nontreponemal tests, with the treponemal tests used to confirm a positive result.
RT-PCR for Treponema pallidum in aqueous humor or vitreous may be useful to confirm syphilitic uveitis [27, 28].
10.4 Differential Diagnosis
Syphilis is one of the great masqueraders of medicine and should be always considered in the differential diagnosis of any intraocular inflammatory disease [6].
10.5 Treatment
Patients with syphilitic uveitis should be considered as having a CNS disease, requiring neurologic dosing regimens regardless of immune status. The recommended treatment is 18–24 million units (MU) of aqueous crystalline penicillin G per day, administered as 3–4 MU intravenously (IV) every 4 h or as a continuous infusion for 10–14 days [10]. Alternatively, ocular syphilis may be treated with 2.4 MU/day of intramuscular procaine penicillin plus probenecid 500 mg four times a day, both for 10–14 days. In the late stage, this may be followed by intramuscular benzathine penicillin G 2.4 MU weekly for up to 3 weeks [9, 10].
The recommended treatment regimen for congenital syphilis in infants during the first months of life is intravenous crystalline penicillin G at 100.000–150.000 units/kg/day, administered as 50.000 units/kg/day every 12 h during the first 7 days of life and every 8 h thereafter, for a total of 10 days [8]. Alternatively, intramuscular procaine penicillin G, 50.000 U/kg in a single daily dose for 10 days may be used.
Alternative treatments in penicillin-allergic patients who show no signs of neurosyphilis and who are HIV negative include doxycycline and tetracycline [9]. Ceftriaxone 2 g IV or IM daily for 10–14 days have been reported to be an effective alternative in patients with ocular syphilis who are penicillin allergic and HIV coinfected [9, 10].
Patients should be monitored for the development of the Jarisch-Herxheimer reaction, a hypersensitivity response of the host to treponemal antigens that are released in large numbers as spirochetes are killed during the first 24 h of treatment [9, 10, 29]. Patients present with constitutional symptoms but may also experience a concomitant increase in the severity of ocular inflammation that may require local and/or systemic corticosteroids.
Topical steroids may be used as an adjunctive treatment in case of keratitis, scleritis, or anterior uveitis. Periocular and/or systemic corticosteroids, appropriately covered with antibiotic therapy, may be useful adjuncts for treating the posterior segment inflammation [30]. Finally, the sexual contacts of the patient must be identified and treated, as a high percentage of these individuals are at risk for developing and transmitting this disease.
Compliance with Ethical Requirements Conflict of Interest The authors declare that they have no conflict of interest. Informed Consent No human studies were carried out by the authors for this article. Animal Studies No animal studies were carried out by the authors for this article.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


