Infections of the Larynx
Vinidh Paleri
Introduction
Laryngeal infections are classified into acute and chronic infections based on the duration of symptoms. Most acute laryngeal infections are caused by viruses and resolve spontaneously within 2 weeks. These occur usually as one of the manifestations of an upper respiratory tract infection. It variably involves the nose and nasopharynx, the oropharynx, and the larynx. The pathogens commonly involved are identified in Table 9.1.
Following a variable prodrome of low-grade fever and malaise, the primary symptoms include sore throat, cough, and a change in voice. The nature of the change in voice can vary from a breathy voice, usually due to the patient protectively splinting the larynx, to a raspy hoarse voice secondary to a haemorrhagic lesion on the cords. The diagnosis is made on the basis of history, general examination, and listening to the voice. Laryngeal inspection is not necessary to confirm the diagnosis. Laryngoscopy will reveal congested vocal cords with prominent vessels and oedema (9.1). Excessive mucus may be evident. Treatment is symptomatic, with advice to rest the voice for at least 48 hours, followed by gentle voicing. However, several infections of the upper aerodigestive tract can present with stridor and airway compromise. A systematic approach is required to achieve the diagnosis and the algorithm shown helps this process (9.2).
Table 9.1 Organisms commonly implicated in acute laryngitis | |
|---|---|
|
 9.1 Acute viral laryngitis as seen through a 70° rigid endoscope, showing congested, oedematous vocal cords. |
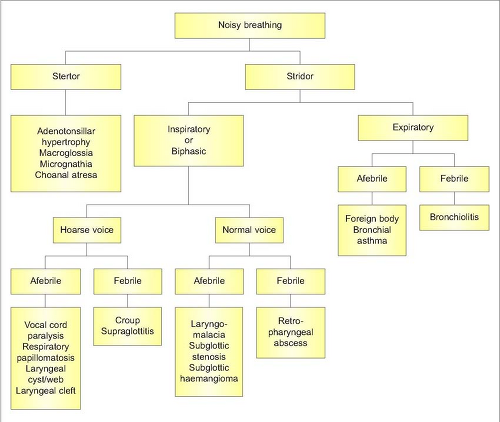 9.2 Algorithm to show the differential diagnosis of stridor in children. (Adapted from Paleri V and Bradley PJ [2007]. Breathing disorders. In: Ludman H and Bradley PJ [eds], ABC of ENT. Blackwell Publishing Ltd, Oxford.) |
Laryngeal infections
SUPRAGLOTTITIS IN CHILDREN
Haemophilus influenzae type B is the usual infective agent, although the incidence has significantly decreased with HiB vaccination. Children between the ages of 2 and 7 years of age are affected, with a peak incidence in 3-year-olds. The disease typically presents with a rapid onset of high fever, toxicity, agitation, stridor, dyspnea, muffled voice, and painful swallowing. Examination will reveal a child in distress, seated, and leaning forward with the mouth open and drooling. If supraglottitis is suspected, no further examination is recommended outside of a controlled setting. In acute supraglottitis, the risk of complete obstruction is high and the airway has to be secured. Endotracheal
intubation is the method of choice as the supraglottic swelling is usually reversible in a few days, unless complications occur. Senior anaesthetic help, with experience in managing the compromised airway, must be sought. An oedematous, cherry red epiglottis with inflammation of the surrounding supraglottis is seen on direct laryngoscopy. Intravenous antibiotics are required.
intubation is the method of choice as the supraglottic swelling is usually reversible in a few days, unless complications occur. Senior anaesthetic help, with experience in managing the compromised airway, must be sought. An oedematous, cherry red epiglottis with inflammation of the surrounding supraglottis is seen on direct laryngoscopy. Intravenous antibiotics are required.
SUPRAGLOTTITIS IN THE ADULT
Although caused by the same infective agent, adult supraglottitis less commonly causes airway distress. Presenting symptoms include fever and acute onset odynophagia, similar to tonsillitis and quinsy. Examination of the oropharynx will be normal or slightly inflamed. Flexible nasendoscopy will clinch the diagnosis when an inflamed supraglottis is evident (9.3). The diagnosis can be missed if laryngeal examination is not performed in adults with acute odynophagia and a normal oropharynx. Management is primarily medical with antibiotics and close observation of the airway. Adult epiglottitis can rarely lead to an epiglottic abscess (9.4). Only 10% of patients will need intubation and intensive care monitoring.
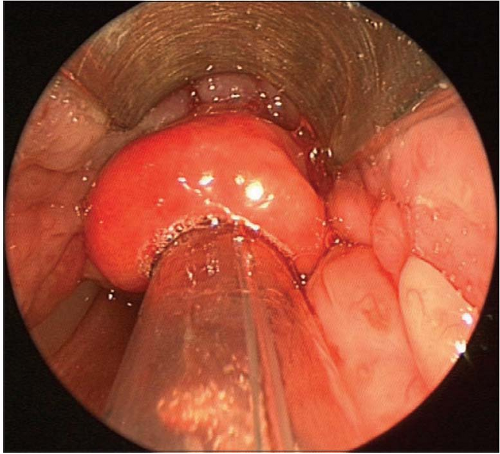 9.3 A rigid endoscopic view of an inflamed and oedematous epiglottis in an adult with supraglottitis. |
 9.4 Flexible endoscopic view of a grossly swollen epiglottis caused by an epiglottic abscess. |
 9.5 The treatment set-up for managing a child with croup. The picture demonstrates a mask in place delivering humidified oxygen and nebulized steroids. Note the saturation monitor and parental presence to calm the child. |
LARYNGOTRACHEOBRONCHITIS (CROUP)
The most common cause of acute stridor in childhood is laryngotracheobronchitis or croup. Parainfluenza virus is the most common causative agent, with influenza virus types A or B, respiratory syncytial virus, and rhinoviruses also being implicated. Children between the ages of 6 months and 3 years are affected, with a peak incidence in the second year of life. A history of preceding upper respiratory tract infection is usually present. Symptoms include low-grade fever, barking cough, inspiratory stridor, and hoarseness. These are characteristically worse at night and are aggravated by agitation and crying. If the diagnosis is clear, no endoscopy is needed. Humidification, oxygen, nebulized steroids, and nebulized adrenaline with systemic steroids are recommended in croup (9.5). Severe cases may need intubation and ventilation for a few days. Recurrent croup should raise the suspicion of congenital subglottic stenosis.
BACTERIAL TRACHEITIS
This is a complication of croup, caused by bacterial superinfection of the trachea. The usual pathogen is Staphylococcus aureus, with others being implicated as well. The presentation is usually that of a croup that does not improve with nebulized epinephrine. High fever, with worsening respiratory distress and chest signs, should alert one to the diagnosis. Treatment involves systemic antibiotics, with tracheobronchoscopy and suctioning of the secretions under general anaesthesia. The majority of patients need intubation and ventilation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


