14
Incorporating Group and Individual Sessions into a Tinnitus Management Clinic
In this chapter, we describe and provide the rationale for each major step of our tinnitus treatment process, including clinical materials and treatment strategies.
The primary goal of our tinnitus treatment program is to equip our patients with the necessary knowledge and tools to promote tinnitus relief by helping them overcome the psychosocial (e.g., depression, concentration difficulty, inability to participate in work and leisure activities) and physical (e.g., sleep deprivation, muscle tension) consequences of tinnitus. Because tinnitus can affect multiple systems (e.g., emotions, physical behaviors), a multidisciplinary team approach is used. Our core team consists of audiologists, otolaryngologists, and psychologists who have a special interest in the treatment of tinnitus. In addition, specialists from other clinical areas, such as a sleep laboratory or pain clinic, may be involved, depending on the individual patient’s needs.
It is important to note that, although we follow several principles of established tinnitus treatment protocols, we do not adhere entirely to one specific management approach. Philosophies from several different disciplines that use a variety of management techniques, including sound therapy, relaxation therapy, biofeedback, and cognitive-behavioral therapy, are incorporated.
Moreover, and somewhat uniquely, clinical services are offered using both group and individual patient contact formats. Including an initial group session prior to individual sessions has added a different, and positive, dimension. There are many advantages for holding group sessions. (The reader is referred to other sources such as Jacobs et al, 1988, and Corey, 1995, for more information on the virtues of group therapy.) Briefly, from the clinician’s viewpoint, conducting group sessions is very cost and time efficient. That is, the same information can be provided to more patients in less time, maximizing available resources. From the patient’s viewpoint, the group experience allows the individual to realize that he or she is not alone, that others suffer from tinnitus as well. The group situation promotes a safe and supportive environment to share experiences with tinnitus and how to cope—or not cope—with the handicapping nature of the tinnitus. Yet an inherent disadvantage of the group setting is the lack of the opportunity to develop the empathic counselor–patient relationship, the one-on-one relationship. It is more efficient to focus on a patient’s specific issues in individual sessions. Therefore, our model for treating tinnitus incorporates both group and individual sessions.
The following sections describe the steps—or visits—in the treatment process. It is important to note, however, that depending on tinnitus severity, it may not be necessary for each patient to participate in all four steps. Therefore, the sequence of visits was developed specifically to assess, diagnose, and treat patients with a wide range of tinnitus severity requiring different levels of management.
Step 1: Initial Diagnostic Evaluations
Audiological Assessment
The first step in the treatment process is to obtain a comprehensive audiological evaluation, including pure-tone and speech audiometry, immittance measurements, and otoacoustic emissions. The audiological evaluation serves three main purposes.
1. The results assist the otolaryngologist in the medical diagnosis of ear disease that may be underlying the tinnitus symptom.
2. Key questions asked during the initial case history (Fig. 14–1) allow the audiologist to assess the severity of the tinnitus and determine if the patient needs to be referred to step 2.
3. Audiological data provide the basis for determining which form of sound therapy should be incorporated in the treatment plan. For example, a patient with a hearing loss may benefit from the use of hearing aids or combination units (hearing aid plus sound generator together in same unit), whereas, an individual with normal hearing may benefit from sound generators alone.
Following the audiological evaluation, patients who are determined to be candidates for step 2 are given a brochure that outlines each step in the management process. Most importantly, patients are counseled strongly about the importance of completing the otolaryngology evaluation and follow-up consultation prior to beginning rehabilitative management.
Medical Assessment
Medical clearance assures the audiologist that there is no underlying pathology that should be addressed prior to the provision of rehabilitative tinnitus management and alleviates the fear held by many patients that they have a serious health condition. Accordingly, the medical evaluation serves both a diagnostic and a therapeutic purpose. It is important that the physician does not provide “negative counseling” to the patient by saying, “Learn to live with it.” Clearly, the physician’s role needs to be positive about the benefits of rehabilitative treatment and to provide reassurance that there is help. This sets the stage for successful management by the audiologist and psychologist on the team.
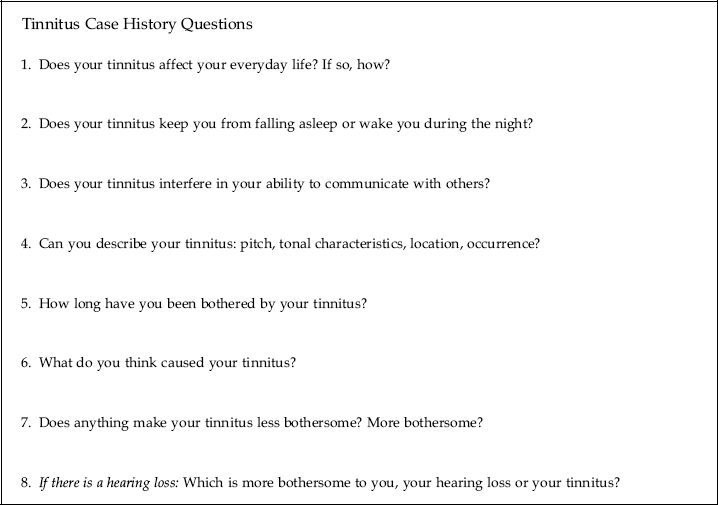
Figure 14–1 Examples of key questions to ask about tinnitus when creating a patient’s case history.
Step 2: Group Education Session
All patients desiring to continue with treatment are scheduled for the group education session. The group format was selected because it is an efficient method of providing informational counseling in a busy clinical practice.
According to Jacobs et al (1988), there are seven different types of groups that are based on their inherent goals: mutual sharing or support groups, discussion groups, task groups, encounter groups, therapy groups, family groups, and education groups. The goal of step 2 is to provide education or informational counseling to a larger number of persons to optimize time and cost efficiency. The optimal size for an education group is up to 12 members (Jacobs et al, 1988). In our group, no more than 8 patients are scheduled per session. Significant others are encouraged to attend and participate. With attrition, the typical size of our groups is 8 to 10 individuals, including significant others. We have found this number of participants to be a very workable size group. It is important to control the group size because too large or too small of a group will inhibit individual participation and reduce opportunities for interaction.
The recommended session length for group therapy is 1½ to 3 hours. Our session is approximately 1½ hours in length—sometimes longer or shorter, depending on the amount of individual participation.
It is very important that confidentiality and privacy be maintained as much as possible during the group. Therefore, we begin each group session warning that information shared in the session is not to be taken out of the room. In addition, each patient signs a shared appointment form (described later).
The information presented in the session is geared toward increasing patients’ understanding of tinnitus and knowledge about management strategies. Although patients are encouraged to share their experiences about their tinnitus, the session needs to be controlled so that individual participants do not use the group as a “sounding board” for their problems. It is critical to the success of the group that each participant understands this important ground rule and that the clinician has the skills to maintain appropriate group dynamics.
The general goals of the group education session are to:
• Clarify misconceptions (e.g., “Will I go deaf because of my tinnitus?”)
• Provide reassurance
• Offer practical suggestions and techniques that provide many patients with immediate relief
• Empower the patient to take control of the tinnitus rather than being controlled by the tinnitus
• Demystify tinnitus by providing an understanding of the mechanisms underlying tinnitus and the rationale for tinnitus relief strategies
• Establish trust and rapport between clinician and patient that will promote compliance with further recommendations
• Provide hope for tinnitus relief
So that patients understand what to expect during the step 2 appointment, a packet of information is sent to them approximately 2 weeks prior to the appointment date. It is important that they realize that this appointment will occur in a group setting, not a one-on-one appointment. Therefore, information explaining the advantages of the group session is provided. It is also important that they realize that the fee for the appointment may not be covered by insurance. The packet of information contains the following items:
• Appointment confirmation letter. This letter briefly summarizes the overall philosophy of the Tinnitus Management Clinic, reminds the patient that he or she must have received medical clearance prior to the group education session, provides a brief outline of the topics to be discussed during the group session, and confirms the date, time, and location of the appointment. Further, patients are informed that there is a fee for the session that is not typically covered by insurance carriers.
• Tinnitus Management Clinic overview fact sheet. This informational piece describes the clinical services provided at each step in the management process along with information about fees.
• Tinnitus Handicap Inventory (THI; Newman et al, 1996). Patients are requested to complete the THI at home prior to the visit. The results of this questionnaire not only assist us in determining the severity of the perceived handicap and serve as a baseline for evaluating future treatment outcome but also allow the patient to realize the extent that the tinnitus affects his or her daily life. That is, a patient indicating minimal handicap on this questionnaire may realize that he or she is indeed coping with the tinnitus and may not need to proceed to the next treatment step. A patient indicating significant handicap may be more motivated to pursue further treatment.
• Shared medical visit waiver. The use of group sessions naturally violates confidentiality; therefore, patients and any significant others are required to sign this waiver. By signing the form, patients agree that “the Cleveland Clinic Foundation shall not be liable for any financial or other damages resulting from any breach of confidentiality committed by other members of the group.” Further more, patients agree “to protect each other’s privacy by not identifying other patients or discussing their health problems outside of the group setting.”
Following check-in, signing of the waiver, and taking care of the financial component, patients are provided a packet of information and escorted to the conference room. The packet of information includes the following:
• A copy of the book Tinnitus: Questions and Answers (Vernon and Tabachnick Sanders, 2001)
• Information about different forms of sound therapy
• An order form for relaxation tapes developed by the Cleveland Clinic Department of Health Psychology and Applied Physiology (available from The Cleveland Clinic/P57, 9500 Euclid Avenue, Cleveland, OH 44195-5189)
• Handouts providing information and Web site addresses for tabletop sound generators (e.g., www.marpac.com), tinnitus relief compact discs (e.g., www.tinnitushelp.com), and other assistive devices (e.g., www.soundpillow.com)
• A membership form for the American Tinnitus Association
The group education session is conducted in a small conference room. All patients and accompanying persons are seated around an oblong conference table. This setting is very informal and promotes good clinician–patient and patient–patient interaction. At the beginning of each session, patients are asked to introduce themselves by first name and provide a brief description of their tinnitus (e.g., When did it start? Where is the tinnitus located? What does their tinnitus sound like?). Following the introductions, the more formal segment of the counseling begins.
The topics addressed in the group education session were selected carefully to be appropriate for a broad range of tinnitus severity. Following is a list of the major topics covered during the group visit.
• Tinnitus definitions
• Epidemiology of tinnitus
• Normal and abnormal anatomy and physiology of the auditory system
• Common reactions to tinnitus
• Overview of treatment options, including sound therapy, cognitive-behavioral therapy, stress management, biofeedback, and relaxation therapy
• Clarification of the remaining steps comprising the treatment we offer
A picture-based presentation using a slide show is used to guide the flow of the discussion. The specific information regarding each of the topics is conveyed using a series of animated picture sequences and sound clips.
At the conclusion of the group education session, the information in the packet provided is reviewed. For many patients, their treatment will end with the conclusion of step 2. Other patients may need to progress to the next steps; therefore, the procedure to schedule the next appointment, step 3, is reviewed. It is important to note that, at this point, continued enrollment is entirely self-selective. That is, it is the responsibility of the patient to decide if further treatment is necessary. Accordingly, the group education session is a process of natural separation for those patients only in need of informational counseling from those who require further evaluation and more intensive individual treatment.
Step 3: Individual Tinnitus Evaluations
Step 3 is initiated when the patient calls to schedule the individual tinnitus evaluation. In response to that call, a set of questionnaires is mailed to the patient along with a return self-addressed stamped envelope. When the completed questionnaires are returned, the appointment is scheduled. The questionnaires serve to assess further the characteristics of the tinnitus (Iowa Tinnitus Questionnaire, Stouffer and Tyler, 1990), assess the urgency for scheduling the psychologic treatment component (Beck Anxiety Inventory, Beck et al, 1997; Beck Depression Inventory-FastScreen for Medical Patient, Beck et al, 1997) and provide the psychologist with information necessary for development of appropriate intervention (Millon Clinical Multiaxial Inventory III, Millon, 1994; Symptom Checklist-90-R, Derogatis, 1977). Each of the aforementioned measures is described briefly in Table 14–1.
The individual tinnitus evaluation phase consists of two major appointments; namely, the individual audiological tinnitus evaluation, conducted in the Section of Audiology, and the individual tinnitus behavioral health assessment, conducted in the Department of Health Psychology and Applied Physiology. If possible, the appointments are scheduled on the same day for patient convenience. The following sections will briefly describe each appointment.
Individual Audiological Tinnitus Evaluation
The individual audiological tinnitus evaluation is a 1½-hour appointment. Tinnitus is evaluated following the World Health Organization (WHO, 1980, 2002) classification scheme for describing the consequences of health conditions (see Table 14–2), as suggested by Tyler (2000). Table 14–2 illustrates the assessment tools used for each domain in the WHO classification scheme. The impairment measures are helpful not only to reassure the patient that the tinnitus is real but also to demonstrate to the significant others what the patient is experiencing (Tyler, 2000). The impairment, disability, and handicap outcome serve as baseline measures against which to assess treatment effectiveness. Furthermore, by conducting an item analysis of the questionnaires, specific problems encountered by the patient may be identified and addressed.
The second component of the individual audiological tinnitus evaluation is the determination of the appropriate sound therapy. All patients are counseled about the importance of maintaining a “sound-enriched” environment and the variety of methods available for maintaining a low-level of background sound. These include the use of tabletop sound generators, special compact disc recordings designed to provide tinnitus relief (e.g., Petroff Audio Technologies DMT-6a Dynamic Tinnitus Mitigation, Palmdale, CA), and/or music. Each of the aforementioned sound generation techniques is demonstrated, along with a discussion of benefits and limitations.
| Iowa Tinnitus Questionnaire. The Iowa Tinnitus Questionnaire (Stouffer and Tyler, 1990) is a 31-item case history form assessing several tinnitus characteristics, including location, tinnitus variability, quality, exacerbating and reducing factors, dysfunctional thoughts, and medication use. In addition, the questionnaire incorporates magnitude estimation rating scales for tinnitus pitch and loudness, annoyance, sleep disturbance, depression, concentration difficulty, and speech interference. |
| The Beck Anxiety Inventory (BAI). This scale is comprised of 21 items evaluating subjective, somatic, and panic-related symptoms of anxiety. The patient is asked to rate how much he or she has been bothered by each of the symptoms (not tinnitus related) listed over the past week on a 4-point (0–3) scale. The items are summed to obtain a total score ranging from 0 to 63 points, with higher scores reflecting greater anxiety. |
| Beck Depression Inventory—FastScreen for Medical Patient. This 7-item scale reflects the cognitive and affective symptoms of depression and is a quick and effective way to screen for depression. For each item the patient is asked to read a group of statements about a single dimension of depression (e.g., pessimism) and to pick out the one statement that best describes how he or she has felt over the past 2 weeks. For example, the responses to the pessimism item include the following statements: I am not discouraged about my future (0 points); I feel more discouraged about my future than I used to be (1 point); I do not expect things to work out for me (2 points); I feel that my future is hopeless and will only get worse (3 points). Scores range from 0 to 21 points, with higher scores reflecting greater perceived depression. |
| The Millon Clinical Multiaxial Inventory-III (MCMI-III). This self-report instrument is composed of 175 true/false items used to identify personality characteristics underlying a patient’s present symptoms and to help guide treatment decisions by providing an integrated picture of personality characteristics. The MCMI-III includes 14 personality pattern scales that coordinate with the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) axis II disorders (e.g., depressive, compulsive, negativistic) and 10 clinical syndrome scales related to DSM-IV axis I disorders (e.g., anxiety, somatoform, post-traumatic stress disorder). |
| The Symptom Checklist-90-R (SCL-90-R). This is a multidimensional self-report inventory designed to screen for a broad range of psychological problems and symptoms of psychopathology and can be used as a measure of treatment progress. The SCL-90-R contains 90 items and can be completed within 12 to 15 minutes. Each of the items is rated on a 5-point scale of distress (0–4) ranging from “not at all” to “extremely.” The scale measures nine primary symptom dimensions (e.g., somatization, hostility, anxiety). There are also three global indices as well: global severity index—designed to measure overall psychological distress; positive symptom distress index—designed to measure the intensity of symptoms; and positive symptom total—reporting the number of self-reported symptoms. |
In addition to the use of nonwearable devices already described, many patients are fit with wearable instrumentation, including ear-level maskers/sound generators, hearing aids, or combination units. Clinic-stock maskers/sound generators are evaluated on the patient in the clinical setting so that they can experience the relief generated by the presence of broadband noise. If the patient has a concomitant hearing loss, the use of a hearing aid alone or a combination unit may be recommended. Determination of the specific device will be based on the results of the audiological and tinnitus evaluation. One tool that has been helpful in determining whether to recommend hearing aids alone or the combination units is the Hearing Handicap Inventory for the Elderly/Adults (HHIE, Ventry and Weinstein, 1982; HHIA, Newman et al, 1990). For example, if the hearing loss has little to no impact on the patient’s psychosocial and communication function (e.g., ≤18 out of 100 points on the HHIE/A), the use of sound generators alone may be indicated. In contrast, if the hearing loss poses significant handicap (>18 points), the use of hearing aids or combination units may be warranted.
| Impairment | Disability/activity limitation | Handicap /participation restriction | |
|---|---|---|---|
| Definition | Dysfunction of auditory system resulting in perception of tinnitus | Reduced abilities of an individual to function in a normal manner as a consequence of the tinnitus impairment | The psychosocial manifestations of and disability that result in the need for extra effort and reduced independence |
| Assessment tools used in our clinic | Psychoacoutic measures: Pitch matching Loudness matching Minimum masking levels Residual inhibition Loudness discomfort levels Magnitude estimation: Pitch estimation Loudness estimation | Iowa Tinnitus Questionnaire Beck Depression Inventory Beck Anxiety Inventory | Tinnitus Handicap Inventory |
| References | Henry et al (2002), Vernon and Meikel (1988) | Stouffer and Tyler (1990) Beck et al (1997) | Newman et al (1996, 1998) |
At the conclusion of the visit, ear mold impressions are taken. The devices are then ordered, and the follow-up appointment is scheduled. The results of the evaluation are documented on a standardized form, allowing a report to be generated within minutes. This report is divided into five main sections: (1) description of the tinnitus, (2) self-report measures results plotted against normative data, (3) summary of the psychoacoustic testing, (4) counseling provided to the patient, and (5) recommendations. Note: The form was designed to include all the tests that we could administer during the assessment appointment; however, in practice, not all tests are administered for each patient. Only those tests completed are recorded.
Individual Tinnitus Behavioral Health Assessment
The psychologist initially conducts a traditional evaluation that includes the psychometric assessment measures described in Table 14–1, the patient’s perspective of his or her tinnitus, a clinical interview, and gathering of personal history. An important part of this evaluation is the process of placing the current tinnitus complaint in the context of any history of psychological distress. Because the appearance of tinnitus symptoms does not take place in a social vacuum, family and relationship information is examined and is quite valuable in eliciting the overall psychosocial context of the patient’s symptomatology.
Step 4: Individual Treatment and Follow-Up
Audiological Management
Patients requiring fitting of devices are seen approximately 2 weeks after the individual audiological evaluation for the fitting of those devices. Because we do not adhere strictly to one specific sound therapy technique for all patients, an individual treatment plan using different levels of sound therapy is devised for each patient based on his or her particular needs. For example, if a patient requires immediate relief from the tinnitus, complete masking is used during the initial treatment phase. That is, a patient with a score on the Tinnitus Handicap Inventory of ≥58 (out of 100 points) may be able to gain some immediate control over the tinnitus and maintain his or her ability to function more normally in everyday life when complete masking is used at the outset. The relief provided by the masking promotes a reduction in stress, which, in our experience, helps to reduce the perception of the tinnitus. Plus, the immediate relief provided by the masking sound gives the patient a sense of hope. Following a short-term period of complete masking (typically 1 month), the patient is “transitioned” into a more long-term management approach using concepts borrowed from the habituation model (Hallam et al, 1984). In terms of the sound therapy regimen, patients are instructed to no longer “cover up” the tinnitus (complete masking) but to set the devices to deliver the sound at a level slightly below the tinnitus (partial masking), facilitating tinnitus habituation. The complete masking phase is only recommended for patients requiring immediate relief. For all other patients, partial masking is the recommended initial phase for sound therapy.
Following the provision of sound generators, hearing aids, or combination units, all patients are scheduled for follow-up appointments at 3 weeks and 3 months. After that, patients are contacted by telephone or e-mail (patient preference) at 6, 12, and 18 months to address questions or concerns. If necessary, patients may return for a face-to-face visit with the audiologist at any time. To monitor progress, the THI is mailed to the patient with a self-addressed envelope at the aforementioned time periods.
Psychological Intervention
Educating the patient in the mind–body connection is a major focus of intervention used by the psychologist. Most patients will readily admit that stress in general, and specifically negative emotions, will exacerbate the intensity of tinnitus. For some, tinnitus symptoms can be triggered by major situational or emotional stress factors that have occurred in their life. The main complaints that patients will attribute to tinnitus during psychological intervention include interference with the onset of sleep, the realization of “no quick cure,” the difficulties of adjusting to having a chronic physical symptom, and the inability to relax secondary to attentional focus on internal tinnitus stimuli.
The most frequent approach used to modify errors in logic and dysfunctional thoughts about tinnitus is cognitive-behavioral therapy. This approach focuses on identifying the connection between thoughts and tinnitus symptoms as well as behavioral factors that may influence the course of tinnitus. The goal of cognitive-behavioral therapy is to reduce depressive self-talk and to reduce unhealthy behavioral risk factors. An example of depressive self-statements is “This isn’t fair. I can’t take this anymore. Why did this happen to me?” An example of unhealthy behavioral risk factors is the intake of high levels of caffeine or tobacco abuse, along with substance abuse. Our belief is that cognitive-behavioral therapy coupled with sound therapy provides a beneficial approach for most patients. That is, any management attempt with sound therapy will be more successful if it is used in conjunction with cognitive-behavioral therapy. In combination, the cognitive-behavioral therapy helps to control the illogical thoughts about tinnitus held by many patients, thereby facilitating habituation.
In addition, we have found that biofeedback and relaxation therapy are effective. Stress is often accompanied by muscle tension, especially tight facial musculature—an example of a frequently occurring mind–body symptom. When this occurs, biofeedback and relaxation therapy would be most beneficial to reduce that muscle tension and, ultimately, the stress.
Utilizing social support is another important psychological treatment intervention in dealing with any type of physical symptom. In the case of tinnitus, social support by family members or significant others often requires education as to the nature of hearing disturbance in general, and tinnitus in particular. The invisibility of tinnitus also makes it difficult for social support networks to understand the degree of interference and distress that can be caused by tinnitus. Therefore, tapes, CD, or computer sound files that simulate tinnitus are often helpful in conveying the annoyance of the tinnitus.
Psychological treatment, although initially viewed with apprehension and reluctance, has been quite effective for our patients with severe self-perceived tinnitus handicap. It is a required component of our treatment for patients to be seen, at least once, by the Department of Health Psychology and Applied Physiology.
Conclusion
Our protocol was designed to provide evaluation and treatment for patients with a broad range of tinnitus severity. Members of the multidisciplinary team offer a variety of strategies to help individuals gain control over their tinnitus and to ultimately improve their quality of life. One unique feature is the group education session. This format offers a cost-effective method for providing important information to tinnitus sufferers. The combination of sound therapy techniques coupled with psychological interventions, including biofeedback, stress reduction, and cognitive-behavioral therapy, has been useful in helping our patients learn to manage their tinnitus.
In this connection, we hope to (1) move tinnitus sufferers from a state of intolerance to a state of tolerance, thereby allowing them to participate in everyday life activities without the constant intrusiveness of the tinnitus; and (2) have patients reach a state where the tinnitus sensation is regarded as a neutral signal rather than one that is disruptive to their lifestyle.
Acknowledgment
We would like to thank Jerome Kiffer for his input regarding the psychological evaluation and treatment section of this chapter and for his continued support of our patients with tinnitus.
References
Beck AT, Guth D, Steer RA, Ball R. Screening for major depression disorders in medical inpatients with the Beck Depression Inventory for Primary Care. Behav Res Therapy 1997;35:785–791
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561–571
Corey G. Theory and practice of group counseling. 4th ed. Pacific Grove, CA: Brooks/Cole; 1995.
Derogatis LR. SCL-90R: Administration, Scoring, and Procedure Manual I. Battimore, MD: Clinical Psychometrics Research; 1997
Hallam RS, Rachman S, Hinchcliffe R. Psychological aspects of tinnitus. In: Rachman S, ed. Contribution to Medical Psychology. Vol 3. Oxford: Pergamon Press; 1984:31–34
Henry JA, Jastreboff MM, Jastreboff PJ, Schechter MA, Fausti SA. Assessment of patients for treatment with tinnitus retraining therapy. J Am Acad Audiol 2002;13:523–544
Jacobs EE, Harvill RL, Masson RL. Group Counseling: Strategies and Skills. Pacific Grove, CA: Brooks/Cole; 1988
Millon T. The Million Clinical Multiaxial Inventory-III (MCMI-II). Minneapolis, MN: National Computer Systems; 1994
Newman CW, Jacobson GP, Spitzer JB. Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg 1996;122:143–148
Newman CW, Sandridge SA, Jacobson GP. Psychometric adequacy of the Tinnitus Handicap Inventory (THI) for evaluating treatment outcome. J Am Acad Audiol 1998;9:153–160
Newman CW, Weinstein BE, Jacobson GP, Hug GA. The Hearing Handicap Inventory for Adults: psychometric adequacy and audiometric correlates. Ear Hear 1990;11:430–433
Stouffer JL, Tyler RS. Characterization of tinnitus by tinnitus patients. J Speech Hear Disord 1990;55:439–453
Tyler R. Tinnitus Handbook. San Diego: Singular; 2000
Ventry IM, Weinstein BE. The Hearing Handicap Inventory for the Elderly: new tool. Ear Hear 1982;3:128–134
Vernon JA, Meikel MB. Measurement of tinnitus: an update. In: Kitahra M, ed. Tinnitus: Pathophysiology and Management. Tokyo: Igaku-Shoin; 1988:36–52
Vernon JA, Tabachnick Sanders S. Tinnitus Questions and Answers. Boston: Allyn & Bacon; 2001
World Health Organization. International Classification of Impairments, Disabilities and Handicaps: A Manual of Classification Relating to the Consequences of Disease. Geneva: Author; 1980
World Health Organization. International Classification of Functioning, Disability and Health (ICIDH-2): Pre-final Draft. Geneva: Author; 2002
< div class='tao-gold-member'>



