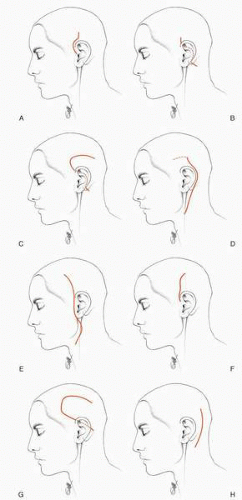
The selection of an incision is based on the need to obtain adequate exposure and to minimize risk and morbidity for the patient. At times the selection may be obvious. For example, for posterior perforations of the tympanic membrane or stapedectomy or the placement of a ventilating tube, the transcanal canal approach is appropriate. However, for other procedures, the surgeon may well have a choice of incisions and approaches. Thus, for example, in chronic otitis media, an attic cholesteatoma without a history of otorrhea may be accessed via an endaural or postauricular incision. The surgeon should consider the advantages and disadvantages of each. Similarly, a small glomus tympanicum tumor, of which the entire circumference is visible on otoscopy, may be adequately accessed by a transcanal incision. On the other hand, a larger glomus tympanicum tumor that extends into the anterior mesotympanum or hypotympanum may well require a postauricular incision for adequate access. The selection of an appropriate incision will include an assessment of the extent of disease using all modalities available to the surgeon, including inspection and preoperative radiographic assessment. A brief listing of surgical incisions and approaches to the external auditory canal, middle ear, mastoid, and lateral cranial base are presented in Table 9.1 and Figure 9.1. The most common incisions for access to the middle ear and external auditory canal are the transcanal, endaural, and postauricular. The postauricular incision may be modified with superior extensions for cochlear implantation. The most common incisions for access to the lateral cranial base include the extended postauricular, preauricular (lateral facial) variations of the transtemporal incision, and the suboccipital incision.
APPROACHES TO THE EXTERNAL AUDITORY, MIDDLE EAR CANAL, AND MASTOID
Transcanal Incisions and Transcanal Tympanomeatal Flap
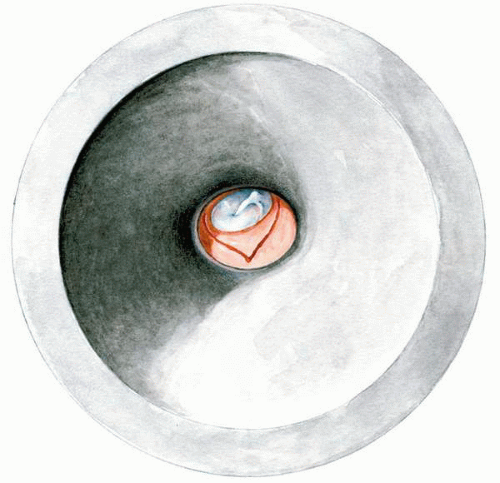
The transcanal approach is appropriate for a variety of surgical procedures limited to the tympanic membrane and posterior tympanic compartment. The most anterior aspect of the tympanic membrane may be hidden by an anterior canal bulge and therefore is better approached by an endaural or postauricular incision. One of the most common surgical procedures done using the transcanal incision is stapedectomy (Chapter 22), in which a transcanal, anteriorly based tympanomeatal incision is used (Fig. 9.2).
With either general or monitored intravenous anesthesia, local injections of an anesthetic are helpful. This is done at two levels, at the meatus of the external auditory canal and in the posterior aspect of the osseous canal. The anesthetic used is 1% xylocaine with a 1:100,000 dilution of epinephrine. After cleaning the external auditory canal, meatal injections are accomplished using a 27-gauge needle in four quadrants—that is, superior, anterior, inferior, and posterior. Following these injections, the meatus may be dilated slightly using a nasal speculum to allow the placement of the largest otologic surgical speculum that can be easily inserted. Using a 30-gauge needle, both superior and inferior injections are then made in the osseous canal several millimeters lateral to the tympanic membrane. This provides anesthesia and hemostasis and facilitates dissection of the cutaneous/periosteal flap from the underlying bone. The most commonly used incisions for creation of an anteriorly based tympanomeatal flap are shown in Figure 9.2. The superior limb should start above the neck of the malleus and extend posteriorly to the mid-tympanic region. This superior limb should always remain several millimeters lateral to the osseous tympanic annulus to provide a sufficient flap width to cover a tympanic ring, which may become enlarged by curettage. The inferior limb should extend anteriorly to a line projected through the axis of the manubrium.
TABLE 9.1Surgical incisions and approaches
Approaches to the External Auditory Canal, Middle Ear, and Mastoid
Suboccipital _ Resection of acoustic neuroma _ Vestibular nerve section
After securing the speculum in a speculum holder, the anteriorly based tympanomeatal flap is elevated using a canal elevator and a 20 F suction tip. Elevation proceeds on a broad front, avoiding “tunneling.” The suction tip should always remain posterior to the elevator and not be allowed to traumatize the flap. Elevation is continued until the fibrous annulus of the tympanic membrane is visualized.
Entry into the middle ear should start superiorly at the posteroinferior limit of the notch of Rivinus, where the fibrous annulus extends anterior to the bony annulus. The fibrous annulus is identified and reflected anteriorly, and the mucosa of the middle ear is incised using either a straight pick or a sickle knife. Elevation of the annulus then proceeds inferiorly either using a sickle knife or annulus elevator, keeping the dissection instrument against the osseous canal to avoid perforation of the drum. A properly elevated tympanomeatal flap will allow visualization of the neck of the malleus superiorly, the manubrium of the malleus in the mesotympanum, and the posterior hypotympanum. The flap is folded over the anterior aspect of the tympanic membrane.
The Endaural Incision
The endaural incision provides excellent expanded access to the tympanic membrane, external auditory canal, and epitympanum. Although these structures may also be accessed via a postauricular incision, the endaural incision has several advantages for both the surgeon and the patient. Thus an endaural incision does not interrupt the majority of the cutaneous innervation of the pinna and therefore does not result in a hypesthetic auricle as does the postauricular incision. In general, the endaural incision does not require postoperative drainage or a mastoid dressing, which is of particular benefit to the patient in an age of outpatient surgery. The endaural incision provides direct access to the epitympanum and external auditory canal. In the postoperative period, following a postauricular incision, the auricle has a tendency to migrate anteriorly, potentially creating a collapsing ear canal, whereas this is not the case with the endaural incision. Thus this author prefers the endaural incision for procedures that predictably involve only the external auditory canal and/or epitympanum, such as anterior atticotomy, canalplasty for exostoses, tympanoplasty for anterior perforations, or total drum replacement. Occasionally an endaural approach may be helpful in middle ear procedures in an abnormally small external canal or meatus. On the other hand, although the endaural approach classically can be used to perform mastoidectomy, particularly with the Heermann extension, if entry into the mastoid compartment is anticipated, the author prefers a postauricular approach.
FIG. 9.1 A: The endaural incision for surgery of the external auditory canal and tympanic membrane. B: The postauricular incision for surgery of the ear canal and tympanomastoid compartment. C: The modified postauricular incision for access to the temporal fossa and for cochlear implantation. D: The extended postauricular incision for access to the tympanomastoid compartment, upper neck, and infratemporal fossa. E: The preauricular (lateral facial) incision for access to the upper neck and infratemporal fossa. F: A preauricular incision for access to the middle fossa surface of the temporal bone. G: A postauricular transtemporal incision for access to the middle fossa surface of the temporal bone. H: The suboccipital incision for access to the posterior fossa.
FIG. 9.2 Incisions for the elevation of a tympanomeatal flap via a transcanal approach.
Only gold members can continue reading. Log In or Register to continue