Fig. 27.1
A graph comparing the aqueous flow across the trabecular meshwork and the inner wall of Schlemm’s canal withand without tension on a Prolene suture in the canal (Reprinted from Tam et al. [90]. With permission from Springer)
Ab interno Schlemm’s canal surgery has also emerged with the premise that if the major resistance point in aqueous outflow is the JTM, devices which result in bypass of this point of resistance should result in lowering of IOP. Although goniotomy in adults and laser trabeculopuncture have been largely unsuccessful as a result of scarring in the surgical area [43–47], new devices such as the trabecular micro-bypass stent (Glaukos Corp., Laguna Hills, California), the Trabectome microelectrocautery device (NeoMedix Corp., San Juan Capistrano, California), and the Hydrus Schlemm’s canal scaffold device (Ivantis Inc., Irvine, California) have been designed to allow aqueous humor to bypass the resistance of the JTM and enter Schlemm’s canal directly. The trabecular micro-bypass stent is a titanium L-shaped half pipe designed to rest in Schlemm’s canal with a snorkel into the anterior chamber [48]. The Trabectome microelectrocautery device is designed with the purpose of removing trabecular meshwork to allow aqueous to directly contact Schlemm’s canal. And finally, the Hydrus microstent is a nitinol alloy scaffold which consists also of an anterior chamber snorkel and intracanalicular segment. Initial studies and clinical data have shown these devices to be effective in IOP reduction and in decreasing the number of glaucoma medications required for IOP control [49–54].
Distal Outflow System
After entrance into Schlemm’s canal and its collector channels, aqueous humor enters the surrounding circulation through aqueous veins and ultimately episcleral and intrascleral venous plexi. The relationship between episcleral venous pressure (EVP) and IOP has been established since the 1950s [55]. As further evidence that elevated IOP was indeed correlated to raised EVP, patients in an inverted posture were found to have an elevated IOP [56]. While the normal EVP varies between individuals, it may range from 8 to 13 mmHg, theoretically being the lowest possible attainable IOP from Schlemm’s canal surgery. Patients with conditions predisposing to elevated EVP such as Sturge–Weber syndrome, venous obstructive disease, and arteriovenous malformations in the orbit, head, neck, or mediastinum are prone to elevated IOP, resulting in glaucomatous optic atrophy [57, 58]. Surgical approaches and attempts at reducing EVP have yet to be described or reported.
Suprachoroidal Outflow
Aqueous humor exits the anterior chamber also via the uveoscleral pathway, consisting of the interstitium of the ciliary body, the suprachoroidal space, and ultimately choroidal and scleral vasculature. Augmentation of outflow via this pathway is achieved using prostaglandin analogs medically and, historically, by creation of a cyclodialysis cleft separation of the ciliary body from the sclera via both ab externo and ab interno approaches [59–63]. Although this often resulted in early successful lowering of IOP, these procedures had several limitations and risks including possible prolonged irreversible hypotony, intraoperative and postoperative hemorrhage due to the vascular nature of uveal tissue, and late closure with scarring of the cleft leading to rapid onset of IOP spikes. One study reported that 75 % of patients undergoing ab interno cyclodialysis cleft creation required further surgical intervention at just 60 days postoperatively [60]. Yet others have attempted to prevent closure and fibrosis of a created cyclodialysis cleft with use of implants such as high molecular weight hyaluronic acid, Teflon tube implants, hydroxyethyl methacrylate capillary strip, and a scleral strip [64–67]. However, these implants have yet to demonstrate successful long-term control of IOP in human eyes with glaucoma. Suprachoroidal seton device implantation has also been reported but likewise without successful long-term control of IOP. Furthermore, implantation of sizeable devices in the suprachoroidal space carries risks of suprachoroidal hemorrhage, choroidal detachment and atrophy, and exudative retinal detachment [68, 69]. The gold suprachoroidal ab externo shunt (SOLX Inc., Waltham, Massachusetts) and the CyPass ab interno microstent (Transcend Medical, Menlo Park, California) are devices designed to provide a pathway for aqueous to travel through and around the shunt from the anterior chamber into the suprachoroidal space to augment uveoscleral outflow. A number of other devices are under development.
The EX-PRESS Shunt: A Subconjunctival Filtration Device
While trabeculectomy has been well established as a potent IOP-lowering procedure, late hypotony, defined as an IOP of less than 6 mmHg at 6 months, has been reported in 42 % of patients [17]. Although a well-established procedure and technically familiar to all glaucoma surgeons, inconsistency even between cases of the same surgeon may yield differing ostium sizes and thus differing amounts of flow. Because of these challenges, as well as the unacceptably high rate of hypotony, the Ex-PRESS Mini Glaucoma Shunt (Optonol Ltd., Neve Ilan, Israel) has been developed to attempt to improve performance and consistency in trabeculectomy.
Four designs of this stainless steel device exist (R–50, X–50, T–50, X–200) with the same functional design, but differing in dimensions and lumen size with the X–200 shunt having a 200-μm-wide lumen while the others with 50-μm lumens (Fig. 27.2). The tip of the shunt consists of one or multiple orifices, which sit in the anterior chamber and allow aqueous to drain through the 27-gauge shaft, designed to approximate the thickness of human sclera. On the underside of the shaft, a spur is present to prevent extrusion of the device out of the anterior chamber, while the scleral side of the shunt consists of an external plate, which prevents the shunt from migrating into the anterior chamber. While the original intent of the shunt was for placement directly under the conjunctiva into the anterior chamber, the high incidence of resultant hypotony, conjunctival erosion, and shunt migration required placement of the shunt under a trabeculectomy style scleral flap [70, 71]. The device appears to be safe in patients undergoing magnetic resonance imaging (MRI) as well as biocompatible to human ocular tissue [72].
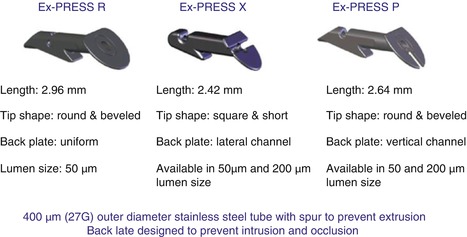
Fig. 27.2
A schematic diagram of the different models of the Ex-PRESS shunt with specifications listed below each
The surgical placement of the shunt begins as if one were to perform a trabeculectomy, with a conjunctival peritomy, gentle cautery, and creation of a scleral flap. Because of the size of the external footplate of the shunt, the scleral flap may have to be slightly larger in dimension than that performed during standard trabeculectomy in order to attain full coverage of the footplate. After the scleral flap has been constructed, the anterior chamber is inflated with viscoelastic or air, particularly in the area where the shunt will be placed. Identification of the scleral spur is critical to the correct placement of the shunt. At the base of the scleral flap, this anatomical landmark should be readily identifiable, and intraoperative gonioscopy can be used to confirm this. At this point, an entry is made into the anterior chamber exactly at the level of the scleral spur with a 27-gauge needle or sapphire blade (manufactured by Optonol) (Fig. 27.3). The angle of entry must be parallel to the iris in order to ensure proper shunt positioning. An entry that is angled toward the iris results in the shunt embedded in the iris, risking incarceration; and likewise an entry toward the cornea may result in shunt–cornea touch and endothelial trauma. The shunt is preloaded on an injector system and is released by the surgeon using the index finger once it has been successfully placed in the previously created needle track entry (Figs. 27.4 and 27.5). Flow through the shunt is then assessed by dry removal of viscoelastic from the anterior chamber using a blunt cannula and irrigation of balanced saline solution (BSS) through the anterior chamber. A peripheral surgical iridectomy is not required. Scleral flap and conjunctival flap closure is then performed in the same manner as standard trabeculectomy. Although the shunt itself is designed to restrict flow, diligent assessment of scleral flap tension must still be performed as excess flow may still occur in the presence of the shunt (Figs. 27.6 and 27.7). Once satisfactory flow has been achieved, watertight conjunctival closure must also be achieved.
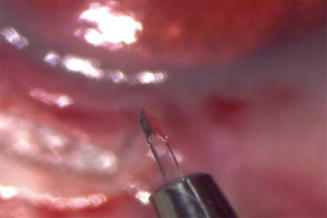

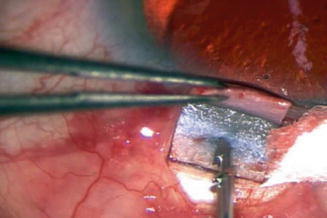
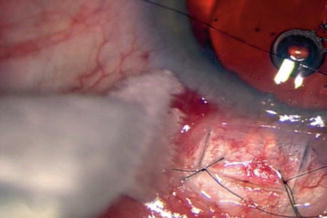
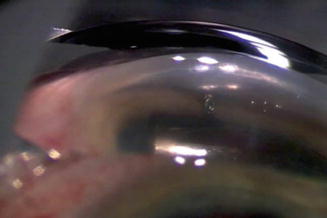
Fig. 27.3
The sapphire blade specifically manufactured for creating the entrance into the anterior chamber for the Ex-PRESS shunt
Fig. 27.4
The handle of the Ex-PRESS shunt injector showing the metal wire under the plastic apparatus that is to be depressed by the surgeon’s index finger when the shunt is to be released from the tip
Fig. 27.5
The Ex-PRESS shunt is inserted into the opening at the level of the scleral spur. Turning the shunt 90° may facilitate its entry
Fig. 27.6
Two interrupted 10-0 nylon sutures are placed into the scleral flap. Tension is adjusted via a slipknot technique. The Ex-PRESS shunt footplate can be seen through the scleral flap with the tip of the shunt visible in the anterior chamber
Fig. 27.7
A gonioscopic view of the Ex-PRESS shunt in the anterior chamber
As the Ex-PRESS shunt relies on a subconjunctival bleb for IOP control, it too may require similar postoperative adjunctive procedures as trabeculectomy such as laser suture lysis and bleb needling with or without antimetabolites. While similar to standard trabeculectomy in the mode of filtration and reliance on a bleb, the Ex-PRESS shunt has the advantages of providing a constant orifice size for filtration, requiring a smaller entry into the anterior chamber, obviating the need for a surgical iridectomy, and providing two-tiered control of IOP via the shunt lumen size and scleral flap tension. It is possible to inject the device in a highly controlled manner [73]. However, despite the design of the shunt to regulate flow, hypotony and overfiltration remain postoperative risks; although when compared to trabeculectomy, some studies have shown that the complication profile, hypotony, and related complications are less frequent in the early postoperative period [70]. Although exclusion criteria advised for the use of the Ex-PRESS shunt includes narrow- and closed-angle glaucoma, it has been our anecdotal experience that it is as well suited for this angle morphology as it is for the open-angle glaucomas.
The Ex-PRESS Mini Glaucoma Shunt is a new device designed to improve the control of IOP and reduce the complication profile of subconjunctival filtration surgery. However, the shunt still relies on a nonphysiologic bleb as the mechanism of IOP lowering, much like trabeculectomy, and therefore the same short-term and long-term complications associated with blebs apply also to the Ex-PRESS shunt. Advantages of the shunt over trabeculectomy include a possibly lowered early postoperative incidence of hypotony, the elimination of the need for a surgical iridectomy, and ease of learning the procedure due to its similarity to performing a standard trabeculectomy. Although it was initially implanted without a scleral flap, the use of a “trabeculectomy-like” flap has made the insertion of this device more appealing [74]. Furthermore, the efficacy of the device has been demonstrated when combined with phacoemulsification [75].
Schlemm’s Canal Devices
Nonpenetrating Ab Externo Schlemm’s Canaloplasty
Canaloplasty is the procedure by which catheterization of Schlemm’s canal is achieved via an ab externo approach in order to restore and enhance physiologic aqueous outflow through the conventional pathway thus avoiding a subconjunctival bleb. Expansion of Schlemm’s canal was first described by Stegmann as viscocanalostomy, a nonpenetrating procedure, wherein two cut ends of the canal were inflated with viscoelastic spanning a few clock hours [35]. Various implants were used in an attempt to enhance the success of nonpenetrating surgery in the early 2000s, but these procedures continued to rely on a bleb for IOP control [37–39]. Recently, a device has been developed to allow 360° cannulation of Schlemm’s canal to expand the entire circumference with viscoelastic and also to allow a suture to be delivered within the canal to exert centripetal force maintaining expansion of the canal. This procedure, termed canaloplasty, aims to restore physiologic outflow via the conventional pathway with suture-assisted canal distension, foregoing the need for a bleb or fistula.
Although in theory Schlemm’s canal can be accessed from any location, the usual chosen surgery site is the superior sclera, for eyelid coverage, in the possible event of bleb formation, as well as for patient comfort. This requires the patient to maintain a down-gaze position for the majority of the procedure. While, in the authors’ experience, topical anesthesia and patient cooperation usually is sufficient for successful performance of the surgery, a traction suture may be utilized to assist in globe positioning and retrobulbar or peribulbar block as well. In some cases, general anesthesia may be required. If a corneal traction suture is utilized, careful site selection is required to ensure the suture is placed several clock hours away from the intended surgical site.
A fornix-based conjunctival peritomy is created, leaving an anterior skirt of conjunctiva attached to the limbus. Blunt dissection is carried out posteriorly to ensure that the posterior edge is relaxed sufficiently to allow for creation of a 5-mm × 5-mm parabolic scleral flap. The posterior conjunctiva should also be easily brought forward to appose to the anterior lip to allow for easy closure at the conclusion of surgery. Light cautery is then applied to the sclera, being careful to avoid aqueous and ciliary veins. Observation of the location of such vessels should also affect the initial selection of where to perform the dissection. A superficial parabolic scleral flap of approximately 5-mm anterior–posterior length by 5-mm width is then outlined on the scleral surface (Fig. 27.8). Although this scleral flap may be any shape, it is the authors’ preference to create a parabolic flap to facilitate watertight closure at the end of surgery. A crescent knife is then used to fashion the superficial flap of approximately one-third scleral thickness (typically 200–300 μm) forward into clear cornea. A deep inner scleral flap is then outlined approximately 1 mm inside from the edge of the superficial scleral flap. Once again, the crescent knife is used to fashion the deep flap and carry it forward directly into Schlemm’s canal. An approximately 100-μm-thick layer of sclera should be left covering the choroid at the base of the deep dissection (Fig. 27.9). It is not uncommon to be left with a full-thickness dissection at some points of the dissection of the deep flap. Care must then be taken to reestablish a tissue plane leaving a thin layer of sclera in the bed of the dissection. It is of utmost importance that the surgeon maintains an adequate depth during the deep flap dissection in order to unroof Schlemm’s canal (Figs. 27.10 and 27.11). If the dissection is too deep, then penetration into the globe occurs, while if the dissection is too superficial, which is more common, it is possible to dissect and pass right over Schlemm’s canal into clear cornea without exposing the canal itself. This results in a difficult situation where a deeper plane of dissection needs to be established with only a thin layer of residual sclera in the bed. Identification of the proper anatomical landmarks is often challenging in these situations, and there is a resultant higher likelihood of penetration into the anterior chamber unintentionally.
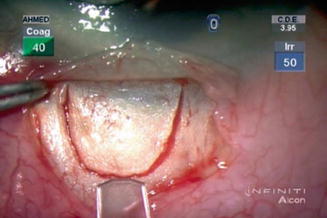
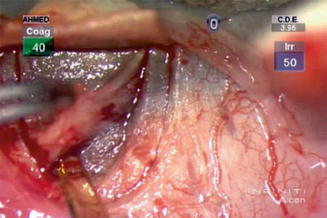
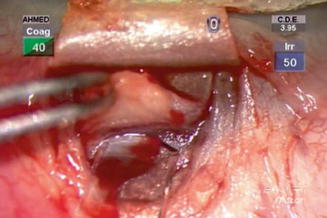
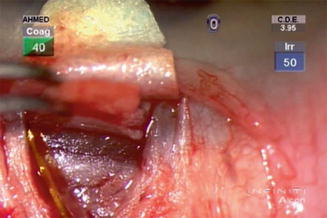
Fig. 27.8
The scleral flap for canaloplasty is outlined in a parabolic shape
Fig. 27.9
After a superficial flap has been fashioned, a deeper scleral flap is created with slightly smaller dimensions than that of the superficial flap
Fig. 27.10
Schlemm’s canal is exposed with a crescent blade
Fig. 27.11
The radial edges of the deep scleral flap are then released being careful not to penetrate into the globe
Once the white limbus-parallel fibers of the scleral spur are visible at the deep dissection, fibers of the outer wall of Schlemm’s canal should be visible by lifting of the deep flap with a toothed forceps. Aqueous humor may be observed to percolate through the Schlemm’s canal, and blood regurgitation may be encountered from the cut ends of the canal (Fig. 27.12). A paracentesis incision should be made in the clear cornea away from the surgical site to lower the IOP to single-digit levels to prevent outward bulging of Descemet’s membrane and the inner wall of Schlemm’s canal, lowering the likelihood of penetration into the anterior chamber during the ensuing delicate dissection. The deep flap is now advanced forward approximately another 1 mm to expose Descemet’s membrane. Aqueous humor may again be observed to percolate through Descemet’s membrane in the anterior bed of the deep dissection commonly known as the trabeculodescemet window (TDW). In some instances, to increase aqueous percolation through the TDW, a Mermoud forceps can be used to delicately strip the inner wall of Schlemm’s canal away. The corneal stroma should be separated from Descemet’s window with surgical sponges such as Merocel (Merocel Corp., North Mystic, Connecticut) and Weck-Cel (Medtronic, Jacksonville, Florida) sponges carefully and gently pushing down on Schwalbe’s line and Descemet’s membrane. Excessive downward pressure, sudden movements, or a dry sponge may easily perforate the TDW and enter the anterior chamber. For this reason, it is the authors’ recommendation that the very tip of the surgical sponges be moistened with a minute amount of balanced saline solution prior to use on the surgical field. Once the TDW has been satisfactorily fashioned, the underside of the deep flap is scored with a sharp-tip blade at the very anterior aspect and cut off with Vannas scissors. Each cut end of Schlemm’s canal is then intubated with a 150-mm outer bore viscocanalostomy cannula, and a very small amount of high viscosity sodium hyaluronate, such as Healon GV (Advanced Medical Optics Inc., Santa Ana, California), is injected into each end to dilate the ostia and facilitate entrance of the iScience device into the canal.
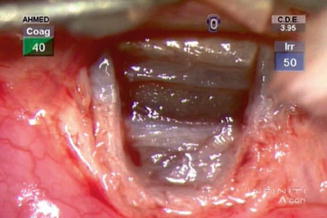
Fig. 27.12
Once the deep flap has been excised, the trabeculodescemet window (TDW) can be seen. Note that heme is emerging from the two cut ends of Schlemm’s canal
In the normal human eye, Schlemm’s canal is known to be of 300 μm in diameter. Studies have shown evidence to suggest that the canal, however, collapses in glaucoma as a result of increased trabecular meshwork and inner wall resistance [76]. A vicious cycle may then be set up, wherein the elevated IOP further compresses Schlemm’s canal because of the reduced circumferential flow of aqueous from the canal into its collector channels. The iScience device aims to restore the patency and re-expand the canal using a 45-mm working length flexible polymer microcatheter of 200-μm shaft diameter with a rounded 250-mm tip diameter designed to be atraumatic to, and to guide the 360° passage and catheterization of, Schlemm’s canal (iScience Interventional Inc., Menlo Park, California). The catheter consists of a central support wire designed to provide a backbone for guidance during advancement and to add resistance to potential kinking of the microcatheter. The optical fibers in the microcatheter allow for transmission of a red blinking light from a laser-based micro-illumination system to the tip to assist in visualization and localization of the tip during passage. Thirdly, the microcatheter possesses a true lumen for the delivery of substances such as viscoelastic to expand the canal during passage or retraction (Fig. 27.13). The proximal end of the device connects to the nonsterile laser-based micro-illumination light source on a mayo stand from one arm, with another arm connected to a sterile screw-mechanism syringe designed to assist in controlled injection of viscoelastic into Schlemm’s canal. The microcatheter is then secured to the surgical drape with surgical tape such as Steri-strips (3 M, St. Paul, Minnesota). Two nontoothed forceps are then used to introduce the microcatheter into one of the cut ends of Schlemm’s canal and advanced 360° until the tip emerges from the other cut end of the canal. Although in the vast majority of patients, this passage is possible, a minority of patients will not allow successful catheter passage through the entirety of the canal. In addition, the authors have observed the microcatheter pass into the suprachoroidal space posterior to Schlemm’s canal. In these cases, early recognition of unusual location of the blinking red light is of utmost importance and the catheter retracted to attempt passage again with scleral depression or removal of the entire microcatheter and passage attempted in the opposite direction.

Fig. 27.13
Once the entire circumference of the canal has been cannulated with the iScience microcatheter, the device is primed with ophthalmic viscosurgical device, which can be seen emerging from the tip of the device on the right
Once the microcatheter has been passed 360° and the tip has emerged, a 10-0 Prolene suture with the needles cut off is tied around the shaft of the device near the tip with the two loose ends tied to the loop (Fig. 27.14). The device is then withdrawn carefully in the reverse direction to which it was passed, with controlled injection of viscoelastic into the canal by a surgical assistant. Care must be taken not to inject an excessive amount of viscoelastic into Schlemm’s canal as a Descemet’s detachment can occur. Regurgitation of heme into the anterior chamber is also commonly seen during passage or withdrawal of the microcatheter. Once the catheter has been removed, the 10-0 Prolene is cut from the tip, essentially leaving two single 10-0 Prolene sutures in the canal with two loose ends emerging from each cut end of Schlemm’s canal. The surgeon must then identify the corresponding ends, and each suture is tied to itself in a slipknot fashion with some back and forth movement in the canal, known as “flossing,” to ensure that the suture sits anteriorly in Schlemm’s canal. Suture tension is then assessed by observing the amount of indentation of the TDW, as well as by pulling the suture knot posteriorly, until it is only barely able to reach the scleral spur (Figs. 27.15 and 27.16). The suture is postulated to produce a surgical pilocarpine-like effect by putting the trabecular meshwork on tension and thus enhancing flow through Schlemm’s canal and its collector channels. Suture tension is felt to play an important role in canaloplasty, where a greater suture tension results in more distension of Schlemm’s canal with resultant greater IOP reduction and increased flow [42].
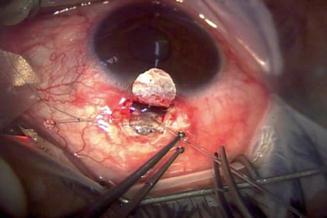
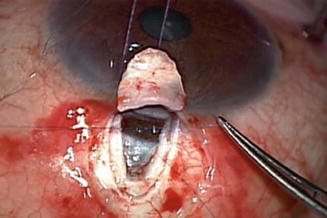
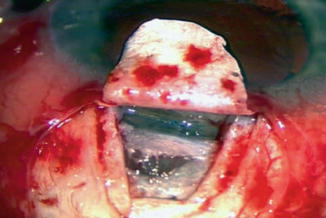
Fig. 27.14
A 10-0 Prolene suture is tied around the end of the device prior to its retraction
Fig. 27.15
Once the suture has been delivered and cut away from the microcatheter, the two cut ends must be matched and tied together
Fig. 27.16
The two suture knots can be seen resting on the TDW
The superficial scleral flap is then placed back into position and sutured in a watertight fashion with five interrupted 10-0 nylon sutures. High viscosity sodium hyaluronate is then injected under the superficial scleral flap using the viscocanalostomy cannula in order to maintain the scleral lake – the space where aqueous humor that has percolated through the TDW accumulates and is then absorbed into episcleral, scleral, and choroidal circulation. The conjunctiva is then closed over the surgical site in a watertight fashion with a 10-0 Vicryl suture in a running horizontal mattress fashion.
Canaloplasty seeks to restore aqueous outflow through the conventional outflow pathway into Schlemm’s canal and its collector channels to control IOP. However, the potential space under the superficial scleral flap, or the scleral lake, also allows for aqueous humor to drain into multiple pathways such as the cut ends of Schlemm’s canal, the surrounding scleral and episcleral vasculature, the suprachoroidal space, and even subconjunctivally in some patients, resulting in a bleb despite a watertight closure. It has been the authors’ experience that fibrosis of the TDW can occur postoperatively with a resultant elevated IOP that requires YAG (yttrium–aluminum–garnet) laser to puncture the TDW, restoring aqueous flow to the scleral lake and resulting in IOP control (Figs. 27.17 and 27.18). A recent study demonstrated that 94 patients who underwent canaloplasty had an IOP reduction from 24.6 to 14.9 mmHg with a decrease in medication usage from 1.9 to 0.6 medications [42]. A similar efficacy was observed in patients undergoing combined phacoemulsification and intraocular lens implantation surgery with canaloplasty [77]. Complications reported were elevated IOP and hyphema, most commonly with Descemet’s detachment, hypotony, and choroidal effusion also being reported.
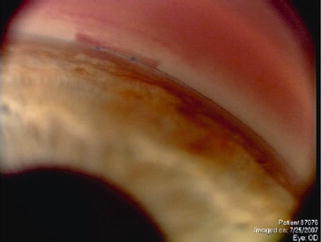
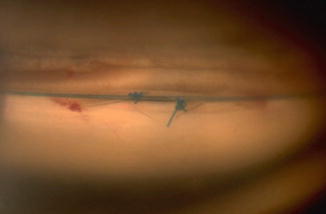
Fig. 27.17
Postoperative gonioscopic photograph of the TDW with the two suture knots
Fig. 27.18
Postoperatively, Nd:YAG laser goniopuncture may be required to break the TDW membrane to augment aqueous egress from the anterior chamber. Note the scrolled edges of the Descemet’s membrane around the suture knots revealing the puncture sites (Reprinted from Tam et al. [90]. With permission from Springer)
Careful patient selection must occur for successful canaloplasty. As the suture in Schlemm’s canal places centripetal tension on the inner wall, it draws the trabecular meshwork in toward the pupil (Fig. 27.19). Although this is a minute distance, in narrow-angle patients or those with crowded anterior segments, this may result in constant or intermittent iridotrabecular touch, peripheral anterior synechiae, and angle closure. As a result, it is advisable to exclude patients with narrow angles or crowded anterior segments from being potential candidates for canaloplasty. Preoperative gonioscopy, and in some cases adjunctive anterior segment imaging, is of great importance in assessing the angle and iris profile when a patient is being considered for this procedure. It has been the authors’ experience that postoperatively even the patient who had an unequivocally open angle may develop peripheral anterior synechiae and iris incarceration into microperforations in the TDW. An intact Schlemm’s canal is also a prerequisite to successful canaloplasty; thus, patients with prior surgery such as a trabeculectomy or patients with obvious scarring in Schlemm’s canal due to prior medication use, laser, surgery, and corneoscleral trauma at the limbus may not be good candidates for canaloplasty.
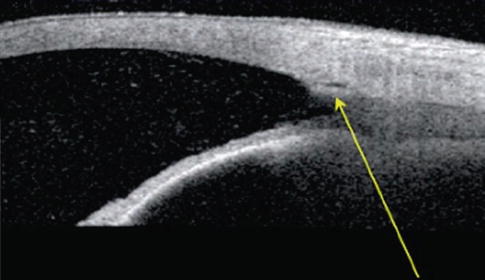
Fig. 27.19
An anterior segment OCT image showing the anterior distension and expansion of Schlemm’s canal induced by the intracanalicular suture (Reprinted from Tam and Ahmed [90]. With permission from Springer)
In summary, canaloplasty is the procedure of catheterizing and distending Schlemm’s canal with an ab externo nonpenetrating dissection and using a microcatheter to deliver viscoelastic and sutures to restore aqueous outflow through the conventional pathway and into a scleral lake created at the surgical site. The aim is to lower IOP in glaucomatous eyes without the reliance on a subconjunctival bleb, thus avoiding both short- and long-term complications of subconjunctival filtration surgery. Studies have shown efficacy at 1 year in terms of IOP reduction and dependence on glaucoma medications with a low complication profile and minimal postoperative management. However, canaloplasty remains technically challenging, and other issues remain to be studied such as the optimal tension of the suture in Schlemm’s canal, the yet-undetermined long-term implications of a suture in the canal, fibrosis of the TDW resulting in the need for postoperative YAG laser, and closure and contraction of the intrascleral lake, and its implications are yet poorly understood. Finally, because of episcleral venous pressure, it would seem that in theory, a ceiling to the maximal amount of physiologic outflow should exist and thus a limit in the lowest IOP attainable by this procedure. This too is yet to be well understood and requires further investigation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


