Purpose
To study the effect of free glasses combined with teacher incentives on in-school glasses wear among Chinese urban migrant children.
Design
Cluster-randomized controlled trial.
Methods
Children with visual acuity (VA) ≤6/12 in either eye owing to refractive error in 94 randomly chosen primary schools underwent randomization by school to receive free glasses, education on their use, and a teacher incentive (Intervention), or glasses prescriptions only (Control). Intervention group teachers received a tablet computer if ≥80% of children given glasses wore them during unannounced visits 6 weeks and 6 months (main outcome) after intervention.
Results
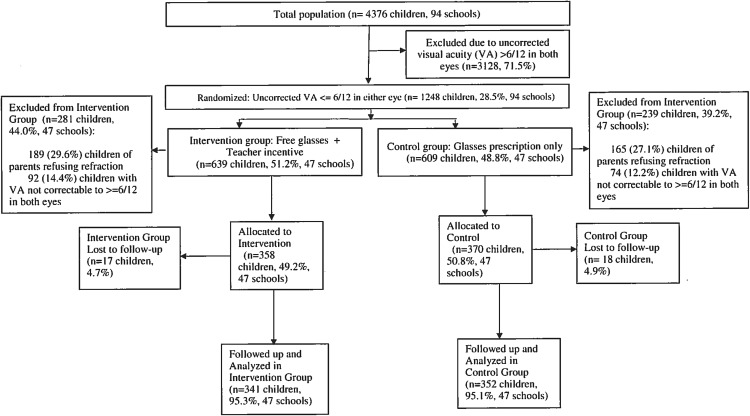
Among 4376 children, 728 (16.7%, mean age 10.9 years, 51.0% boys) met enrollment criteria and were randomly allocated, 358 (49.2%, 47 schools) to Intervention and 370 (50.8%, 47 schools) to Control. Among these, 693 children (95.2%) completed the study and underwent analysis. Spectacle wear was significantly higher at 6 months among Intervention children (Observed [main outcome]: 68.3% vs 23.9%, adjusted odds ratio [OR] = 11.5, 95% confidence interval [CI] 5.91–22.5, P < .001; Self-reported: 90.6% vs 32.1%, OR = 43.7, 95% CI = 21.7–88.5, P < .001). Other predictors of observed wear at 6 months included baseline spectacle wear ( P < .001), uncorrected VA <6/18 ( P = .01), and parental spectacle wear ( P = .02). The 6-month observed wear rate was only 41% among similar-aged children provided free glasses in our previous trial without teacher incentives.
Conclusions
Free spectacles and teacher incentives maintain classroom wear in the large majority of children needing glasses over a school year. Low wear among Control children demonstrates the need for interventions.
Uncorrected refractive error is the leading cause of visual disability among children worldwide, affecting nearly 13 million under the age of 16 years, among whom nearly half live in China. If not treated, refractive error is associated with loss of visual function and reduced educational performance in children. Though refractive error can be safely and inexpensively managed with glasses, as few as 1 in 6 children needing spectacles have them in rural parts of the developing world.
Spectacle distribution programs for children can lead to normalization of visual function and trial-proven, significant improvements in educational outcomes. However, programs in China, Mexico, and Africa have reported poor compliance with free spectacles, with rates of observed, short-term wear at unannounced visits ranging from 13% to 41%. Factors limiting wear of glasses include discomfort or inconvenience, concerns over being teased, parental opposition, lack of perceived need, and fear of damage to the eyes (though a trial has now demonstrated that spectacle wear is in fact protective against age-related declines in uncorrected visual acuity among children). Previous randomized trials of specially designed educational interventions promoting spectacle wear aimed at children, teachers, and parents have demonstrated very modest or no impact on observed use of glasses among children at unannounced follow-up visits.
We carried out a cluster-randomized controlled trial among children at predominantly migrant schools in urban eastern China, to determine whether providing free glasses combined with education on their use and a teacher incentive could lead to improvements in observed spectacle wear among children at unannounced visits over the course of a school year. Comparison is also made in the current report to rates of observed wear over similar time periods among similar-aged children receiving free spectacles under an identical protocol in a previous published trial, without the use of teacher incentives. Our hypothesis was that the combination of free spectacles and teacher incentives would maintain compliance with classroom spectacle wear, where impact on educational attainment is presumably greatest, in the majority of Incentive group children over the course of a school year.
Methods
The protocol for this cluster-randomized trial was prospectively approved in full by institutional review boards at Stanford University (Palo Alto, California, USA) and the Zhongshan Ophthalmic Center (Guangzhou, China). Permission was received from local boards of education in each setting, and from the principals of all schools, and at least 1 parent provided written informed consent for the participation of each child. The principles of the Declaration of Helsinki were followed throughout. This trial was registered at http://isrctn.org , under the registration number ISRCTN16720066.
Setting
The study was carried out in Shanghai (the world’s largest city, with a total municipal population of 24.2 million in 2012, including 9.6 million migrants) and Suzhou/Wuxi (“twin cities” located near Shanghai, with a combined prefectural population of 17.0 million in 2014, half estimated to be migrants). These cities were selected for having among China’s largest populations of migrants, a term defined in this study as including families who did not have a local primary residence ( hukou ), implying reduced access to local public health care and schools. Substantial rural and suburban areas exist within the borders of all of these cities, and migrant populations tend to be clustered in these rural/suburban zones. In these communities migrant children mostly attend schools that are private and unregulated, with little support from the government.
Sampling and Eligibility Criteria
All elementary schools in these cities identified by the local Bureaus of Education as having a primarily migrant population were enumerated and 94 schools were selected at random (66 in Shanghai and 28 in Suzhou/Wuxi). One fifth grade class (children aged 10–12 years) was selected at random in each school, and questionnaires (see below) were administered and visual acuity testing and refraction (see below) carried out. All children in the selected classes meeting both the following visual and refractive criteria were eligible: uncorrected visual acuity ≤6/12 in either eye; refractive error meeting cutoffs shown to be associated with significantly greater improvement in visual acuity when corrected : myopia ≤−0.75 diopters (D), hyperopia ≥+2.00 D, or astigmatism (nonspherical refractive error) ≥1.00 D.
Questionnaires
At baseline (September 2013, beginning of the school year), enumerators administered questionnaires to children concerning their age, their sex, urban vs rural residence, whether they were an only child, glasses wear, belief that wearing glasses harms vision (a common misapprehension in China), family migrant status, and parental glasses wear, education, and place of residence/work (local vs elsewhere). A study-specific mathematics test was administered as an index of academic achievement. Teachers were asked to state whether the blackboard (potentially not clearly seen by myopic children and so a possible driver of glasses use) was used for all, most, about half, little, or none of teaching. A parental questionnaire asked about ownership of 14 selected items as an index of family wealth. Children were told to bring their spectacles on the day of the baseline examination, and baseline spectacle use was defined as being able to produce glasses at school.
Visual Acuity Assessment
Children underwent baseline visual acuity screening at school by a nurse and trained assistant. Visual acuity was tested separately for each eye without refraction at 4 meters using an Early Treatment Diabetic Retinopathy Study chart (Precision Vision, La Salle, Illinois, USA) in a well-lighted, indoor area. If the orientation of at least 4 of 5 optotypes on the 6/60 line was correctly identified, children were examined on the 6/30 line, on the 6/15 line, and then line by line to 6/3. Visual acuity for an eye was defined as the lowest line on which 4 of 5 optotypes were read correctly. If the top line could not be read at 4 meters, the subject was tested as above at 1 meter, and the measured visual acuity was divided by 4.
Refraction
Children with uncorrected visual acuity ≤6/12 in either eye underwent cycloplegia with up to 3 drops each of cyclopentolate 1% and proparacaine hydrochloride 0.5%. Children then underwent automated refraction (Topcon KR 8900; Topcon, Tokyo, Japan) with subjective refinement by a local optometrist, previously trained by experienced optometrists from Zhongshan Ophthalmic Center.
Randomization and Interventions
This was a cluster-randomized, controlled trial, with schools as the clusters ( Figure ). The trial was originally designed to include 150 schools and to include 3 treatment arms (control, free glasses, and free glasses combined with teacher incentive). However, in view of lower-than-expected enrollment and our having recently completed a large trial providing glasses only to similar-aged children, the glasses-only arm was dropped. In October 2013, after the baseline survey and vision screening but prior to refraction, eligible children were randomized by school to receive 1 of 2 interventions:
- •
Free spectacles based on the child’s measured refractive power dispensed at school by the study optometrist. A letter informing the parents about the free glasses program and including the child’s prescription was sent to parents, and a previously described educational intervention directed at teachers and children and promoting spectacle wear was carried out. Additionally, teachers (but not children) in eligible classes were informed that if ≥80% of children given glasses were wearing them at the time of 2 unannounced class visits, the teacher would receive a tablet computer (approximate value US$350; approximate monthly teacher income US$450). This offer was made to Chinese, mathematics, and English teachers (the main academic subjects in Chinese primary schools) (Intervention group, 47 schools); or
- •
A glasses prescription and letter to the parents informing them of the refractive status of their child, with free glasses provided only at the conclusion of the trial, though this was not previously announced. No teacher incentive was offered. (Control group, 47 schools).
Randomization was carried out at a central location (Stanford University, Stanford, California, USA) using R software (R Foundation for Statistical Computing, Vienna, Austria). Participants (students, parents, and teachers) and enumerators were not informed of either the overall design of the study or the explicit treatment arm assignment.
Educational Intervention
The educational intervention has been described elsewhere in detail. Children at Intervention group schools watched a video and were given cartoon-based pamphlets and a classroom presentation showing children experiencing the benefits of glasses and teachers explaining that glasses do not harm vision. Teachers viewed a presentation at school on the safety and benefits of glasses, accompanied by a brochure with similar information, and posters with similar content were hung in classrooms.
Outcome Assessment: Glasses Wear
Trained assessment teams consisting of 2 persons each returned unannounced to each school at 6 weeks and 6 months after distribution of glasses and prescriptions. At these visits, spectacle wear was assessed through unannounced direct examination. The main study outcome was observed wear (that is, glasses actually present on the child’s face) at 6 months, and the secondary outcome was self-reported wear at 6 months, assessed on the same occasion. After completing the unannounced direct examination, enumerators also asked sampled children in each school to describe their own spectacle wear (secondary outcome) as “always,” “only for studying,” or “usually not worn.” These study personnel were masked to children’s group assignment.
Sample Size
Power calculations were performed using Optimal Design software ( http://sitemaker.umich.edu/group-based/optimal_design_software ) for cluster-randomization and binary outcome (wear vs non-wear). Based on our earlier trials in similar-aged children, we assumed an estimated rate of wear of 30% in the Control and 70% in the Intervention group, and a 20% prevalence of myopia. We determined that 90 schools (45 per group) with 1 class per school (an average of 50 children, with 10 expected to have myopia) would provide 90% power to detect the expected difference between groups with an alpha error of 0.05, intraclass correlation of 0.15.
Statistical Methods
We standardized baseline math score to give a mean of 0 and standard deviation (SD) of 1. Baseline wear of glasses was defined as being able to produce glasses at school, having been told the day before to bring them, whereas a positive self-report of wear at follow-up was defined as wearing glasses “Always” or “Only for studying.” We calculated family wealth by summing the value, as reported in the China Rural Household Survey Yearbook (Department of Rural Surveys, National Bureau of Statistics of China, 2013), of items on the list of 14 owned by the family. Refractive power was defined throughout as the spherical equivalent, spherical power plus half the cylindrical power.
Subsequent to randomization, a number of children either could not undergo refraction owing to parental refusal of cycloplegia or did not meet our refractive and visual criteria to receive glasses (see above). Thus, our analyses were performed in per-protocol fashion using the vce (cluster) command in Stata 12.0 (StataCorp, College Station, Texas, USA), calculating robust standard errors to adjust for clustering by school. Our analysis took 2 forms. In the primary analysis, we used logistic regression to examine the association between baseline variables and observed wear at unannounced visits 6 weeks and 6 months (main outcome) after provision of spectacles and prescriptions. Second, we used multiple logistic regression to determine whether membership in the Intervention group was associated with observed spectacle wear at 6 weeks and 6 months, adjusting for other baseline factors. These included variables associated with 6 week/6 month wear at P ≤ .20 (baseline spectacle wear, baseline uncorrected VA, baseline math score, parental education, family migrant status, and parental glasses wear) and those we felt important to adjust for on a theoretical basis (age, sex, rural vs urban residence, status as an only child, belief that wearing glasses harms the vision, family wealth, and blackboard use).
Missing Data
To reduce the inefficiency of estimation owing to missing values, we use multiple imputation in Stata to impute data for several data at baseline: rural residence (n = 17), beliefs about the potential harm of wearing glasses (n = 4), baseline glasses wear (n = 1), parental education (n = 10), having both parents working in the area (n = 5), and family wealth (n = 55). We used logistic regression for binary variables and ordered logistic regression for ordinal variables. The independent variables used for imputation included all nonmissing variables listed in Table 1 . The multiple imputation approach created 20 copies of the data in which missing values were imputed by chained equations. Final results of multivariate analysis were obtained by averaging these 20 datasets using Rubin’s rules, which ensured that the standard errors for all regression coefficients took into account uncertainty in the imputations and in the estimation.
| Variable | Control Group (n = 370 at 47 Schools) | Intervention Group (n = 358 at 47 Schools) | P Value, Control vs Intervention | Missing Data, Number (%) |
|---|---|---|---|---|
| Age, y, Mean (SD) | 11.0 (1.0) | 10.9 (0.9) | .80 | 0 (0.0) |
| Male sex (n, %) | 191 (51.6) | 180 (50.3) | .71 | 0 (0.0) |
| Rural residence (n, %) | 320 (88.2) | 295 (84.8) | .26 | 17 (2.3) |
| Only child in family (n, %) | 74 (20.0) | 70 (19.6) | .91 | 0 (0.0) |
| Believes wearing glasses harms vision (n, %) | 127 (34.5) | 118 (33.1) | .72 | 4 (0.5) |
| Wearing glasses at baseline (n, %) a | 66 (17.8) | 64 (17.9) | .98 | 1 (0.1) |
| VA <6/18 both eyes (n, %) | 164 (44.3) | 142 (39.7) | .24 | 0 (0.0) |
| Math score, mean, SD | 0.1 (1.0) | 0.2 (1.0) | .83 | 0 (0.0) |
| At least 1 parent with >12 years education (n, %) | 112 (30.7) | 108 (30.6) | .98 | 10 (1.4) |
| Both parents working in the area (n, %) | 323 (87.8) | 299 (84.2) | .18 | 5 (0.8) |
| At least 1 parent wears glasses (n, %) | 65 (17.6) | 70 (19.6) | .56 | 1 (0.1) |
| Family wealth (n, %) | .14 | 55 (8.0) | ||
| Top tercile | 101 (29.4) | 114 (35.1) | ||
| Middle tercile | 120 (35.0) | 110 (33.8) | ||
| Bottom tercile | 122 (35.6) | 101 (31.1) | ||
| Blackboard use (n, %) | .52 | 0 (0.0) | ||
| < Half of teaching | 12 (25.5) | 16 (34.0) | ||
| Half of teaching | 19 (40.4) | 16 (34.0) | ||
| > Half of teaching | 16 (34.0) | 15 (31.9) |
a Defined as being able to produce glasses at school, having been told the day before to bring them.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


