Purpose
To assess in uveitis patients the rate of immunosuppressive drug (ISD) discontinuation in real-life clinical practice, comparing this rate among ISDs.
Design
Longitudinal retrospective cohort study.
Methods
We included uveitis patients attending a tertiary eye referral center from Madrid (Spain) between 1989 and 2015, prescribed any ISDs (cyclosporine, methotrexate, azathioprine, anti-TNF drugs, or others). Our main outcome was discontinuation of all ISDs owing to clinical efficacy, inefficacy, adverse drug reaction (ADR), and other medical causes. Discontinuation rates (DRs) per 100 patient-years were estimated. Variables associated with specific-cause discontinuations were analyzed using Cox bivariate and multivariate models.
Results
We analyzed 110 patients with 263 treatment courses and 665.2 patient-years of observation. Cyclosporine (66.4%), methotrexate (47.3%), azathioprine (30.9%), and anti-TNFs (30.9%) were the most frequently used ISDs. Treatment was suspended in 136 cases (mostly owing to clinical efficacy [38.2%], inefficacy [26.5%], and ADRs [22.8%]). All-cause DR with 95% confidence interval was 20.4 [17.3–24.2]. Retention rates at 1 and 10 years were 74% and 16%, respectively. In the multivariate analysis, combined treatment exhibited higher DRs owing to clinical efficacy than other ISDs in monotherapy. Conversely, nonbiologic combination therapy with azathioprine exhibited the highest DR owing to ADRs.
Conclusions
Clinical efficacy was the most frequent cause for ISD discontinuation, followed by inefficacy and ADRs. DR owing to efficacy was higher for combination therapy. Furthermore, nonbiologic combination therapy with azathioprine was associated with a higher DR owing to ADRs.
Uveitis comprises a diverse group of inflammatory diseases affecting the uvea and adjacent tissues. Its exact pathogenesis is unclear, but evidence suggests an immune-mediated cause for noninfectious uveitis.
Uveitis patients are at risk for developing substantial and sometimes permanent visual loss, and uveitis is the third most common cause of vision impairment in the developed world, accounting for 10%–15% of all cases of total blindness. Therefore, its correct management is essential for preserving visual function and avoiding ocular and extraocular morbidity. Patients are usually treated based on the presence of signs of inflammatory activity using a stepwise protocol, corticosteroids being its cornerstone. However, in case of inadequate response (incomplete response to high doses and/or inability to maintain control of inflammation with low doses) and/or dose-dependent side effects, the addition of immunosuppressive drugs (ISDs) is needed to achieve a sustained control of the inflammatory process and/or to reduce corticosteroid use. Furthermore, certain conditions benefit from an early initiation of these therapies.
Most of the data regarding efficacy, tolerability, and discontinuation rates (DRs) of ISDs in uveitis patients come from clinical trials. However, trial settings are different from day-to-day clinical practice, limiting the validity of the extrapolated data to patients in daily practice. Furthermore, data from observational studies in uveitis are scarce.
The objective of our work was to describe the rate of ISD discontinuation in real-life clinical practice using a cohort of uveitis patients attending a tertiary care outpatient clinic, to compare the DRs among the most frequent ISDs used, and to analyze the influence of several demographic and disease-related variables in the DRs.
Methods
We performed a longitudinal retrospective cohort study, with subjects included between October 1989 and November 2015 and followed up until December 31, 2015, with a maximum follow-up time of 26 years. Patients were collected from the Hospital Clinico San Carlos Uveitis Clinic (HCSC-UC), a tertiary eye referral center in Madrid (Spain), composed of a multidisciplinary team of ophthalmologists and rheumatologists ( Supplementary Text , Setting Description ; Supplemental Material available at AJO.com ). This study was approved as a retrospective study by the Hospital Clinico San Carlos Ethics Review Board, and waiver of informed consent was obtained for use of deidentified clinical records. Furthermore, the study was conducted in accordance with the Declaration of Helsinki.
Patient Sample and Data Collection
We included consecutive patients that: (1) have attended the HCSC-UC, (2) were clinically diagnosed with noninfectious uveitis based on an expert ophthalmologic examination, (3) were prescribed with any ISDs (including cyclosporine [CSA], methotrexate [MTX], azathioprine [AZA], anti-TNF therapy [anti-TNF: including infliximab, adalimumab, etanercept, and golimumab], cyclophosphamide, mycophenolate, tacrolimus, or tozilizumab), and (4) for whom the dates of prescription and discontinuation of the ISDs were registered on the patient’s clinical record.
We excluded from the analysis those patients (1) diagnosed with scleritis, episcleritis, pemphigoid, or optic neuritis, (2) in whom the ISD treatment was prescribed owing to extraocular manifestations of an associated systemic disease and not the uveitis itself, and (3) who received treatment with ISDs before they attended our clinic and no information regarding date of prescription and/or discontinuation was registered in their clinical records.
Clinical records were reviewed in January 2016 and demographic and disease-related data extracted, including the dates on which all ISDs were first prescribed, dates suspended, and the reason for discontinuation. If a patient was still receiving an ISD when the data were collected, they were recorded as continuing such treatment.
Variables
Our main outcome was all ISD discontinuation owing to: (1) inefficacy as ophthalmologist/rheumatologist criteria (the physician’s impression that the current treatment failed to improve inflammation or relapses occurred despite the therapy), (2) clinical efficacy as ophthalmologist/rheumatologist criteria (the physician’s impression that the treatment could be discontinued owing to lack of inflammatory activity during a certain period of time), (3) adverse drug reactions (ADRs), defined as an injury related to medical management, and (4) other medical causes (including pregnancy, patient decision, change of diagnosis, and elective surgeries).
The ISD treatment was analyzed as a categorical variable based on the particular ISD or combination prescribed (“CSA in monotherapy,” “MTX in monotherapy,” “AZA in monotherapy,” “anti-TNF in monotherapy,” “biologic and nonbiologic therapy in combination,” “nonbiologic therapy in combination,” “other ISDs in monotherapy”). It is important to consider that owing to the small numbers and shorter follow-up times of each particular biologic therapy, we decided to group all these medication into 1 category. Several covariates were considered, including demographic, disease-related (uveitis diagnosis and other clinical characteristics such as course and location, and information regarding visual acuity [VA] and inflammatory activity at the beginning of each treatment course [defined as the period of time in which a particular ISD or combination was prescribed], such as presence of cells in the anterior chamber, vitreous haze, retinal vasculitis, chorioretinitis, cystoid macular edema [CME], or epiretinal membrane [ERM]), pharmacologic-related (such as concomitant treatment with corticosteroids), and previous ISD discontinuation ( Supplementary Text , Variables Description , section A).
Statistical Analysis
Continuous variables were described using median and interquartile range (IQR). Dichotomous and categorical variables were described using proportions. ISD all-cause and specific-cause crude DRs were estimated by dividing the number of events occurring during the time of observation by the number of person-years of exposure, and given per 100 person-years with 95% confidence intervals (CI).
The time of observation comprised the elapsed time from the date the first ISD was prescribed (or, in those subjects that received ISDs in multiple periods, the date any ISD was prescribed again after the last discontinuation; to be considered 2 different periods for the same ISD or combination, more than 30 days had to have elapsed between discontinuation and reintroduction of the same ISDs) until the occurrence of any of the following cutoff points: loss of follow-up, main outcome, or the end of the study (December 31, 2015). The time of observation was subsequently divided into successive periods, defined by a particular combination of ISDs (treatment courses).
All-cause and specific-cause discontinuations were multiple-event variables, meaning that the same patient could experience the same main outcomes several times during follow-up.
Kaplan-Meier curves were set to account for discontinuations. Bivariate and multivariate Cox regression models were constructed to assess the influence of demographic and disease-related variables in the risk of specific-cause discontinuations.
Models that included the variables “presence of CME,” “ERM,” “cells in anterior chamber,” or “vitreous haze” were also adjusted by the variable “OCT availability/SUN criteria” (see Supplementary Text , Variables Description , section B).
Age, sex, calendar time, and those variables with a P value <.15 in the bivariate analysis were included in the multivariate analysis. Different models were compared using the likelihood-ratio test, in order to select the fittest model to the data. Results were expressed as hazard ratio (HR) and 95% CIs. To account for the influence of the different diagnosis of uveitis in ISD discontinuation, all models were stratified by uveitis diagnosis.
Regarding missing data, for categorical variables a dummy category for such missing observations was included, so they could be included in the analysis. Continuous variables were categorized using quartiles and a dummy category for those observations with missing data was included.
Proportional-hazard assumption was tested using Schoenfeld residuals and the scaled Schoenfeld residuals. In the multivariate models, those variables that did not meet this assumption were removed unless the global model fulfilled such assumption.
Models for each main outcome were adjusted using the Bonferroni method. Taking into account that we analyzed the influence of 29 variables in each main outcome, the P value threshold for significance was .0017. Several sensitivity analyses were also carried out to ease comparison with previous studies of ISD discontinuation (see Supplementary Text , Sensitivity Analysis ).
Analyses were performed using STATA 12 software (Stata Corp, College Station, TX, US).
Results
Cohort Description
We identified 145 patients treated with ISDs between 1989 and 2015. We excluded 10 patients diagnosed with other inflammatory eye diseases; 8 patients treated with ISDs owing to extraocular manifestations; and 17 patients lacking information regarding dates of prescription or discontinuation. We included in our study 110 patients, with a total follow-up time of 665.2 patient-years and a median (IQR) follow-up time per patient of 4.4 years (2.5–9.1). Demographic and clinical characteristics are shown in Table 1 .
| Variable | Result (N = 110) |
|---|---|
| Women, n (%) | 69 (62.7) |
| Age at first ISD prescribed, median (IQR) | 34.9 (24.7–49.1) |
| Year when the first ISD was prescribed, n (%) | |
| <2000 | 28 (25.5) |
| 2000–2007 | 32 (29.1) |
| 2008–2015 | 50 (45.5) |
| Elapsed time from first visit to first ISDs, n (%) | |
| Before first visit in our clinic | 37 (33.6) |
| First month | 23 (20.9) |
| 2–6 months | 18 (16.4) |
| 7–12 months | 9 (8.2) |
| >12 months | 23 (20.9) |
| Spaniard, n (%) | 98 (89.1) |
| Lateratity, n (%) | |
| Unilateral | 21 (19.1) |
| Bilateral | 89 (80.9) |
| Course, n (%) | |
| Acute no relapsing | 7 (6.4) |
| Acute relapsing | 49 (44.6) |
| Chronic | 54 (49.1) |
| Location, n (%) | |
| Anterior | 6 (5.5) |
| Intermediate | 30 (27.3) |
| Posterior | 32 (29.1) |
| Panuveitis | 42 (38.2) |
| Diagnosis, n (%) | |
| Primary intermediate uveitis | 25 (22.7) |
| Ophthalmologic chorioretinitis | 23 (20.9) |
| Primary panuveitis | 16 (14.5) |
| Behçet disease | 15 (13.6) |
| Primary vascular retinitis | 11 (10.0) |
| Vogt-Koyanagi-Harada syndrome | 7 (6.4) |
| Others | 13 (11.8) |
| Pattern, n (%) | |
| Acute recurrent unilateral AU | 1 (1.0) |
| Acute bilateral AU | 1 (1.0) |
| Chronic AU | 4 (3.6) |
| Intermediate uveitis | 30 (27.3) |
| Unilateral chorioretinitis | 2 (1.8) |
| Bilateral chorioretinitis | 14 (12.7) |
| Retinal vasculitis | 16 (14.6) |
| Panuveitis with chorioretinitis | 14 (12.7) |
| Panuveitis with retinal vasculitis | 21 (19.1) |
| Panuveitis with exudative retinal detachment | 7 (6.4) |
| Systemic disease, n (%) | |
| Behçet | 15 (13.6) |
| Vogt-Koyanagi-Harada | 7 (6.4) |
| Sarcoidosis | 4 (3.6) |
| Multiple sclerosis | 4 (3.6) |
| Juvenile arthritis | 3 (2.7) |
| Others | 5 (4.5) |
Only the disease-related variables assessing VA and inflammatory state showed missing data, with 15.6%–25.1% of missing observations ( Supplementary Table 1 ; Supplemental Material available at AJO.com ).
CSA was the most used drug (73 patients; 66.4%), followed by MTX (52; 47.3%), anti-TNFs (34; 30.9%), AZA (34; 30.9%), and other ISDs (9; 8.2%). Considering each drug separately and that each patient could receive the same drug several times, we registered 228 uses of ISDs ( Supplementary Table 2 ; Supplemental Material available at AJO.com ). Considering the particular ISD or combination prescribed, we observed 263 treatment courses: 190 (72.2%) in monotherapy, 66 (25.1%) with 2 ISDs, and 7 (2.7%) with 3 drugs. The most frequent course was CSA in monotherapy (79 courses; 30.0%), followed by MTX in monotherapy (52; 19.8%), biologic and nonbiologic ISDs in combination (47; 17.9%), AZA in monotherapy (33; 12.6%), nonbiologic ISDs in combination (26; 9.9%), anti-TNFs in monotherapy (21; 8.0%), and other ISDs (5; 1.9%). For more information, see Supplementary Text, Results (a) .
All-Cause and Specific-Cause Discontinuation Rates
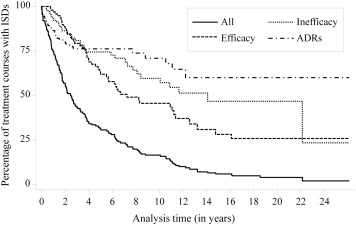
Overall, treatment courses ended in suspension in 136 occasions, mainly owing to clinical efficacy (52 patients; 38.2%), inefficacy (36; 26.5%), ADRs (31; 22.8%), and other medical causes (17; 12.5%). The most frequent ADRs were digestive (mostly gastrointestinal intolerance: 10, 32.3%), increase of liver enzymes (6, 19.4%), deterioration of renal function (6, 19.4%), and infections (3, 9.7%).
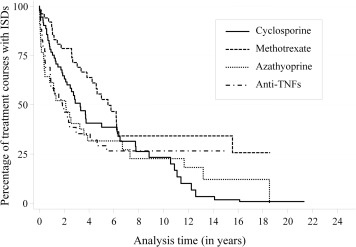
The median survival rate (with 95% CIs) was 2.5 [1.8–3.3] years, and the retention rates (with 95% CIs) for 1, 5, 10, and 15 years were 74% [65–81], 31% [24–39], 16% [11–23], and 6% [3–10], respectively. The overall crude rates with 95% CIs for all-cause and specific-cause discontinuations (clinical efficacy, inefficacy, ADRs, and other causes) per 100 patient-years were 20.4 [17.3–24.2], 7.8 [6.0–10.3], 5.4 [3.9–7.5], 4.7 [3.3–6.6], and 2.6 [1.6–4.1], respectively ( Figure 1 ). When we compared the rates for all-cause discontinuation among ISDs ( Figure 2 ), we observed that anti-TNFs had the greatest rate (21.7 [14.9–31.6]), followed by AZA (20.5 [14.1–29.7]), CSA (19.7 [15.0–25.8]), and MTX (10.7 [7.3–15.6]). Table 2 shows the cause-specific DRs for each ISD. We observed that anti-TNFs, AZA, and CSA exhibited the highest DRs owing to clinical efficacy, inefficacy, and ADRs, respectively ( Supplementary Figures 1–3 ; Supplemental Material available at AJO.com ). Cause-specific DRs for particular ISDs or combinations are shown in Supplementary Table 3 (Supplemental Material available at AJO.com ).
| Therapy | Follow-up | Improvement | Inefficacy | Adverse Event | |||
|---|---|---|---|---|---|---|---|
| Failures | DR [95% CI] | Failures | DR [95% CI] | Failures | DR [95% CI] | ||
| Cyclosporine | 264.2 | 19 | 7.2 [4.6–11.3] | 12 | 4.5 [2.6–8.0] | 17 | 6.4 [4.0–10.4] |
| Methotrexate | 252.7 | 13 | 5.1 [3.0–8.9] | 4 | 1.6 [0.6–4.2] | 4 | 1.6 [0.6–4.2] |
| Azathioprine | 136.6 | 5 | 3.7 [1.5–8.8] | 11 | 8.1 [4.5–14.5] | 8 | 5.9 [2.9–11.7] |
| Anti-TNFs | 124.7 | 14 | 11.2 [6.7–19.0] | 8 | 6.4 [3.2–12.8] | 3 | 2.4 [0.8–7.5] |
Influence of Demographic and Disease-Related Variables in Specific-Cause Discontinuation Rates
Results from the bivariate Cox regression analysis can be found in Supplementary Tables 4–7 (Supplemental Material available at AJO.com ). In the multivariate analysis ( Table 3 , and Supplementary Tables 8–10 ; Supplemental Material available at AJO.com ), we observed that a previous suspension owing to clinical efficacy was significantly and independently associated with a lower rate of discontinuation owing to clinical efficacy. Additionally, monotherapy with anti-TNFs was associated with a higher risk of discontinuation owing to clinical efficacy when compared with monotherapy with CSA, MTX, or AZA ( P = 1.3 × 10 −4 , P = 4.5 × 10 −4 , and P = 1.2 × 10 −4 , respectively). Also, combined therapy was associated with higher DRs, but differences became statistically significant only when compared with AZA, the ISD with the lowest DR (vs biologic and nonbiologic drug combination: P = 3.2 × 10 −4 ; vs nonbiologic drug combination: P = 1.5 × 10 −3 ). No differences were observed among monotherapy with anti-TNFs and combined therapy with or without biologic drugs.
| Improvement | Inefficacy | Adverse Drug Reaction | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HR [95% CI] | P | q a | HR [95% CI] | P | q a | HR [95% CI] | P | q a | |
| Women | 0.66 [0.3–1.46] | .30 | 0.98 | 1.52 [0.6–3.82] | .38 | 0.44 | 1.04 [0.39–2.75] | .94 | 0.41 |
| Age at course | |||||||||
| <17 | Ref. | – | – | Ref. | – | – | Ref. | – | – |
| 17–29 | 5.85 [1.05–32.56] | .044 | 0.54 | 0.67 [0.12–3.9] | .66 | 0.68 | 3.14 [0.24–41.55] | .39 | 0.92 |
| 30–55 | 2.69 [0.48–15.03] | .26 | 0.59 | 0.26 [0.04–1.59] | .14 | 0.77 | 1.76 [0.14–22.3] | .66 | 0.93 |
| >55 | 1.69 [0.24–11.93] | .60 | 0.54 | 0.85 [0.13–5.79] | .87 | 0.89 | 3.07 [0.23–41.7] | .40 | 0.93 |
| Year at course | |||||||||
| Before 2000 | Ref. | – | – | Ref. | – | – | Ref. | – | – |
| 2000–2007 | 0.98 [0.32 to 3] | 0.97 | 0.011 | 0.76 [0.21–2.7] | .67 | 0.82 | 2.31 [0.63–8.5] | .21 | 0.76 |
| 2008–2015 | 0.75 [0.24 to 2.28] | 0.61 | 0.19 | 0.56 [0.08–3.93] | .56 | 0.59 | 1.16 [0.14–9.8] | .89 | 0.98 |
| Unilateral | 3.36 [1.34 to 8.44] | 9.80×10 −3 | 0.43 | – | – | – | – | – | – |
| Systemic disease | – | – | – | – | – | – | 26.02 [3.74–180.82] | 9.80 × 10 −4 b | 0.89 |
| Vasculitis | 2.13 [0.82=5.53] | .12 | 0.34 | – | – | – | – | – | – |
| Cystoid macular edema | – | – | – | 3.53 [1.18–10.53] | .024 | 0.63 | – | – | – |
| Treatment during cycle | |||||||||
| Cyclosporine in monotherapy | Ref. | – | – | Ref. | – | – | Ref. | – | – |
| Methotrexate in monotherapy | 1.1 [0.32–3.82] | .88 | 0.97 | 0.86 [0.16–4.5] | .86 | 0.90 | 0.19 [0.04–0.85] | .030 | 0.38 |
| Azathioprine in monotherapy | 0.3 [0.06–1.49] | .14 | 0.017 | 2.76 [0.79–9.7] | .11 | 0.53 | 1.12 [0.34–3.69] | .85 | 0.66 |
| Anti-TNF in monotherapy | 17.94 [4.09–78.62] | 1.30 × 10 −4 b | 0.88 | 1.35 [0.12–14.85] | .81 | 0.48 | No failures | – | – |
| Anti-TNF and nonbiologic ISDs in combination | 6.39 [1.93–21.17] | 2.40E-03 | 0.84 | 6.83 [1.66–28.07] | 7.70 × 10 −3 | 0.27 | 0.34 [0.07–1.77] | .20 | 0.52 |
| Nonbiologic ISDs in combination | 6.02 [1.59–22.88] | 8.40E-03 | 0.076 | 6.92 [1.82–26.26] | 4.50 × 10 −3 | 0.61 | 4.08 [1.15–14.45] | .029 | 0.33 |
| Others | No failures | – | – | 2.61 [0.23–29.61] | .44 | 0.50 | No failures | – | – |
| Previous suspension owing to clinical improvement | 0.09 [0.03–0.33] | 2.20 × 10 −4 b | 0.48 | – | – | – | – | – | – |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


