From a radiologic workup perspective, tinnitus is classified into pulsatile, which can be objective, and nonpulsatile, which is typically subjective. There is considerable discrepancy within the literature regarding the percentage of positive findings in patients with pulsatile tinnitus. The authors discuss the overlap in the radiographic findings detected in association with tinnitus in both asymptomatic patients and symptomatic patients and the importance for imaging to detect treatable causes. They discuss imaging related to diagnosis and treatment and provide an imaging workup algorithm.
Tinnitus is the experience of auditory sensation in the absence of external stimuli. In the western countries, it is estimated that 12% of the population is affected by tinnitus to varying degrees. Most patients present in the seventh to eighth decade of life .
Many classification schemes for tinnitus are available. Many investigators characterize tinnitus according to subjective or objective, and pulsatile or nonpulsatile. Others evaluate pitch or loudness of the noise. Pulsatile tinnitus coincides with the patient’s heartbeat. Nonpulsatile tinnitus does not and can be either intermittent or continuous. Tinnitus can be subjective (experienced by the patient only) or objective (perceptible to another). Full neurotologic clinical examination typically precedes imaging workup. Clinically, pulsatile tinnitus can further be divided into arterial or venous origin. Differentiation between the two can be made by applying pressure over the ipsilateral internal jugular vein (IJV). This maneuver usually has no effect on the intensity of the arterial type, whereas the venous type should subside with this technique .
From a radiologic workup perspective, tinnitus is classified into pulsatile, which can be objective, and nonpulsatile, which is typically subjective. There is considerable discrepancy within the literature regarding the percentage of positive findings in patients with pulsatile tinnitus. Weissman and Hirsch found that most patients with subjective tinnitus and normal otoscopic examination have no imaging abnormalities to explain the tinnitus. Sonmez and colleagues described radiographic abnormalities in 61.9% of patients with subjective tinnitus; however, it remains unclear whether these positive abnormalities were the cause of the subjective tinnitus or incidentally found.
In objective pulsatile tinnitus, Weissman and Hirsch found that most patients have no imaging abnormalities while Sonmez and colleagues postulated that radiographic abnormalities can be detected in up to 100% of patients and De Ridder and colleagues have found 15% of patients with pulsatile tinnitus have no imaging abnormality. The variability of the results is likely because of the uncertainty as to whether the radiographic findings are indeed the etiology of the patient’s tinnitus or just incidental findings. For example, Sonmez and colleagues considered jugular bulb variants as positive findings in patients with tinnitus. However, jugular bulb venous variants are common findings and can be seen in asymptomatic patients. It is unclear what percentage of these imaging abnormalities were indeed the cause of tinnitus in these patients and a very large study would be necessary to have enough statistical power to truly determine the relationship between relatively common normal variants and clinical symptoms. The goal of imaging is to identify treatable causes of tinnitus.
Many radiologic findings associated with tinnitus have been seen in asymptomatic patients. Koesling and colleagues presented a review of 223 thin-section CT temporal bone scans where only 5% of these patients were referred for tinnitus. They detected the following vascular variations: mastoid emissary vein (82%), lateral sigmoid sinus (28%), high-riding jugular bulb (6%), and anterior sigmoid sinus (55%). Less than 1% showed persistent stapedial artery, aberrant internal carotid artery, jugular bulb diverticulum, and dehiscent sigmoid sinus. All of these findings have been seen in asymptomatic patients as well as in patients with tinnitus . Therefore, it is critical to correlate the radiographic findings with the full neurotological exam and the overall clinical picture .
Imaging workup algorithm
When an imaging abnormality is found in pulsatile tinnitus, it is usually from a vascular mass (neoplasm), vascular malformation, or bony/developmental abnormality of the middle ear cavity and otic capsule where MRI is less sensitive .
Imaging of objective pulsatile tinnitus begins with contrast-enhanced temporal bone CT .
If the examination is normal and clinical suspicion is high, then consider conventional angiography to evaluate for dural arteriovenous fistula or malformation. If both studies are normal or if there is low suspicion for dural vascular abnormality, then consider enhanced CT of the neck through the superior mediastinum to look for venous compression or CT angiography of the neck to evaluate for atherosclerotic disease.
Imaging of subjective pulsatile tinnitus begins with contrast-enhanced temporal bone CT .
If this study is normal, then consider contrast-enhanced CT of the neck through the superior mediastinum to look for venous compression or atherosclerotic disease.
Imaging of nonpulsatile tinnitus begins with MRI of the internal auditory canal with intravenous contrast .
Refer to Box 1 for Imaging Protocols from University of Pittsburgh Medical Center.
Contrast-enhanced temporal bone CT :
- •
64 detector row CT scanner
- •
125 cc nonionic contrast with 60-second delay for both arterial and venous opacification
- •
Kvp 120, mA 280, slice thickness 0.625 mm
- •
Coronal reconstructions
MRI of the IAC (1.5T):
- •
Brain: 5-mm axial fluid attenuated inversion recovery (FLAIR), T1-weighted sagittal images, and contrast-enhanced fat-suppressed T1-weighted axial images.
- •
IAC: 2- to 3-mm T1-weighted axial and coronal images (pre and post contrast enhancement), and high-resolution thin-section three-dimensional (3D) T2-weighted axial images, using either Fast Spin Echo or fast imaging employing steady state acquisition techniques (FIESTA).
Pulsatile tinnitus
Neoplasm
Glomus tumors, or paragangliomas, are benign vascular neoplasms that arise from paraganglia that follow the cranial nerves. The most common paragangliomas that present with pulsatile tinnitus are the glomus tympanicum, glomus jugulare, and glomus jugulotympanicum, which is a glomus jugulare that has grown into the middle ear.
Glomus tympanicum are the most common tumors of the middle ear cavity and arise along the medial middle ear cavity along the course of Jacobson’s nerve, a branch of the glossopharyngeal nerve (CN 9). Typically they occur along the cochlear promontory but can occur throughout the mesotympanum along the course of Jacobson’s nerve. Glomus tumors may also arise from Arnold’s nerve, a branch of the Vagus nerve (CN10), which enters the facial canal to course along the facial nerve. They appear as red retrotympanic pulsatile masses on otoscopic exam ( Fig. 1 ) .
Glomus jugulare tumors arise from the paraganglia of the adventitia at the jugular bulb. They grow superiorly into the middle ear cavity and then can be visible on otoscopic exam. CT scan can show early characteristic moth-eaten or permeative erosive changes of the jugular foramen. Glomus jugulare tumors can avidly enhance and be indistinguishable from normal jugular vein making the inferior extent difficult to define. Moreover, it can invade the lumen of the jugular vein. There can be variable signals within the jugular vein that may reflect slow flow, turbulent flow, or tumor involvement, which can be difficult to distinguish on MRI . MRI may show a salt-and-pepper appearance to the lesion illustrating the multiple flow voids of the tumor; however, this is not always present. The classic described “salt-and-pepper” appearance is seen on long TR/TE images. The “pepper” component represents flow void while the “salt” component represents hyperintense foci due to slow flow or hemorrhage. This is usually seen in glomus tumors greater than 1 cm ( Figs. 2 and 3 ) .
Hemangiomas within the internal auditory canal are rare. They are typically hyperintense on T1- and T2-weighted MR images but there have been reports of either isointensity or hypointensity on T1-weighted images. They typically show strong enhancement patterns. When large, they can demonstrate stippled calcifications, although it is not the rule. When stippled calcifications are present, they may help differentiate hemangioma from schwannoma . Depending on location and the nerve of origin, these lesions can cause severe and progressive sensorineural hearing loss, tinnitus, facial nerve palsy, or vertigo . Hemangiomas can occur anywhere along the facial nerve. When they occur at the geniculate ganglion, patients typically present with facial nerve dysfunction (96%) and rarely hearing loss (5%) . Hemangiomas found in the internal auditory canal have a higher rate of hearing loss with variable degrees of hearing loss . When they do occur in the internal auditory canal, they typically involve the facial nerve.
Vascular malformation
A dural arteriovenous fistula or arteriovenous malformation is the most frequent cause of objective pulsatile tinnitus in patients with a normal otoscopic exam . Any dural sinus may be involved, but the two most frequent sinuses involved are the cavernous sinus and the transverse sinus. The dural arteriovenous fistula to most commonly cause pulsatile tinnitus is in the transverse sinus region. CT or MRI are often normal but may demonstrate too many or enlarged vascular structures including cortical veins, and the sigmoid or transverse sinuses. Conventional angiography remains the gold standard for this diagnosis ( Fig. 4 ) .
Vascular anomalies
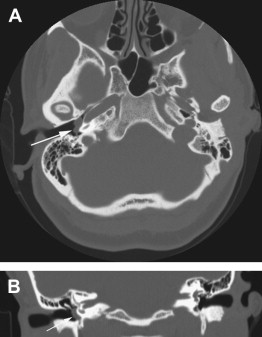
An aberrant internal carotid artery is not the true internal carotid artery but rather a hypertrophied inferior tympanic artery that arises from the ascending pharyngeal branch of the external carotid artery. The inferior tympanic artery enlarges to anastomose with the caroticotympanic artery in the middle ear and resumes the course of the petrous internal carotid artery. Along the way, the inferior tympanic canaliculus enlarges and resembles the carotid canal. It may or may not be dehiscent in the middle ear. This occurs in response to a carotid artery that never develops. CT scan will show the dehiscence and abnormal course of the vessel into the middle ear. Magnetic resonance angiography (MRA) and conventional angiography will show the abnormal lateral course of the aberrant carotid artery. Often, it may be best appreciated on CT since one can see the bony landmarks .
The persistent stapedial artery can occur with an aberrant internal carotid artery or with a normal carotid artery. It is persistence of a fetal circulation that courses between the crura of the stapes (obturator foramen) then courses along the tympanic segment of the facial nerve and exits to supply the middle meningeal artery territory. It generally regresses with birth . When there is a persistent stapedial artery, the middle meningeal artery does not develop and thus there is no foramen spinosum. These abnormalities can be seen on thin-section CT scan. The persistent stapedial artery is likely too small to be seen on MRA .
Redundant anterior inferior cerebellar artery has been implicated by some authors as an etiology of tinnitus. Vascular contact with the cisternal segment of the vestibulocochlear nerve has been associated with nonpulsatile tinnitus while vascular contact with cranial nerve (CN) 8 in the internal auditory canal has been associated with pulsatile tinnitus . De Ridder and colleagues postulate that the etiology of pulsatile tinnitus may be caused by direct transmission of pulsation to the cochlea via the internal auditory canal. They further state that the pulsations are heard via a so-called bone conduction mechanism, rather than via cochlear nerve compression. It is well known that intrameatal vascular loops can be present without generating pulsatile tinnitus. Potentially, the sharpness of the vascular loop as well as the size of the internal auditory canal may be contributory to the development of tinnitus. Furthermore, these authors postulate that the reason we do not hear our carotid arteries as they course through the petrous bone is the presence of a perivenous plexus that surrounds the carotid and is most prominent between the carotid artery and the cochlea. The venous plexus acts as a sound barrier and dampens the acoustic effect of the carotid .
Improvement in tinnitus has been described with microvascular decompression of the CN 8. However, many patients are scanned for other reasons that have vessels in close proximity to the CN 8 without symptoms of tinnitus. MRI optimally illustrates this finding ( Fig. 5 ).



