Imaging of the Temporal Bone
Hugh D. Curtin
Osamu Sakai
Imaging has become an integral part of the evaluation of many otologic problems (1, 2, 3). Computed tomography (CT) and magnetic resonance imaging (MRI) are the primary tools of modern imaging of the temporal bone. The appropriate modality depends on the clinical problem because these imaging systems provide very different information. Because the anatomy and pathology clearly shown by one modality may be completely invisible in the other, design of the imaging plan is of obvious importance.
This chapter is not a complete description of lesions involving the temporal bone. Rather, we will provide a strategy for imaging in various clinical situations and show the landmarks and findings that are most important in making decisions. Radiologists may vary in the selection of an approach to arrive at the information considered most important. Ongoing consultation and interaction between clinician and radiologist contribute significantly to the evolution of an appropriate imaging strategy.
COMPUTED TOMOGRAPHY AND MAGNETIC RESONANCE IMAGING
Although the technical details of MRI and CT imaging are inappropriate in this review, a few key terms and concepts will help the otolaryngologist to appreciate the strengths and limitations of each approach.
Computed tomography is based on electron density and follows the same principles as plain film radiography. Denser structures such as metal and bone stop more X-rays and therefore are white on the image, whereas less dense structures stop fewer and are darker or black. Most soft tissues are intermediate in density and are shown as various shades of gray. Muscle, tumor, and fluids all approximate the same density. Fat is substantially lower density and is darker than other soft tissues on CT. Iodinated contrast has a very high electron density and so makes any tissue or space that can be reached by the contrast more opaque or “whiter” than before the contrast is administered. Thus a tumor that has a blood supply will be whiter after injection of intravenous contrast than before. Contrast injected intrathecally opacifies the cerebrospinal fluid (CSF), which therefore appears white.
Bone and soft tissue algorithms are computer programs applied to the raw data obtained from the actual scan. These computer manipulations give additional information without additional radiation.
One of the most recent innovations in CT technology is the multidetector spiral CT machine. The use of multiple detectors allows extremely thin, direct scan images and the production of excellent multiplanar reformatted images. For instance, the computer takes the information from a direct axial image set and produces high resolution images in the coronal or sagittal plane. The resolution is the same in the reformatted image as in a directly acquired image. This technique gives the capability of high resolution reformatted images in any plane without the need for additional radiation to the patient.
Magnetic resonance imaging, as currently practiced, relies on the magnetic properties of hydrogen nuclei. A radio frequency is used to stimulate the nuclei and a sensitive antenna detects the signal emitted as the nuclei “relax”—that is, return to their normal state. The terms T1 and T2 refer to different types of relaxation of the nuclei. One of the most obvious findings of a T1-weighted image is that fat has a very high signal and is therefore white on the image. Fluid such as CSF has a low signal and is dark but not black. Cortical bone and air have virtually no signal and so typically appear as true black. Various soft tissues appear as shades of gray. Intravenous gadolinium increases the signal, or brightness, of any vascularized tissue. Thus tissue (e.g., many solid tumors) is “brighter” on the postcontrast T1-weighted image than on a similar sequence performed prior to contrast.
T2-weighted images show low protein fluids such as CSF as a high signal (bright). Fat is usually dark. Newer, fast spin echo T2-weighted sequences, however, show fat as bright unless fat suppression is used, which results in a dark T2 appearance.
One of the advantages of MRI is the seemingly unending nuances that can be applied in modern sequence design. For example, fast flowing blood causes a black “signal void” on many sequences. However, other sequences can be made very sensitive to any type of movement and can show flow as bright. These specialized sequences are the basis of MR angiography. The fat signal is a key part of evaluating head and neck tumors. However, the high signal of fat can interfere with appreciation of subtle enhancement of various tumors and inflammation. Special fat suppression techniques can be added, allowing better visualization of even minimal enhancement adjacent to fat.
Although the great variety of available sequences provide more information, the varying appearances can be quite confusing when one first tries to work with MRI. Most imaging centers develop relatively standard protocols.
In otologic imaging the preferred modality depends on the region to be assessed. Cortical bone and air have the same appearance on MRI. Because neither gives signal, both appear black in the image. The ossicles are invisible in a normally aerated middle ear. With CT, bone and air are almost at the opposite ends of the density spectrum and so clear delineation of these structures is possible. With CT, soft tissue and fluid are different from bone and from air and so one can identify small amounts of fluid and soft tissue in the middle ear and mastoid region. For these reasons CT is usually the first study done for evaluation of the external auditory canal, middle ear, and mastoid.
Computed tomography and MR can both be used for imaging of the inner ear. Computed tomography emphasizes bone, showing the contours of the otic capsule and demonstrating the fluid-filled spaces as lucencies. Magnetic resonance imaging demonstrates the fluid directly with the bone represented by a signal void. In the internal auditory canal, MRI becomes the clear choice. High resolution MRI can show the actual nerves crossing the fluid of the internal auditory canal or can demonstrate subtle enhancement of a small tumor. The densities, even with enhancement, are not great enough for CT to reliably separate the structures in the canal.
CLINICAL AND REGIONAL EVALUATION
The radiologist must tailor the examination to the clinical presentation and expected diagnosis. Although there is overlap, an initial approach divides the temporal bone into several major regions. Imaging then is refined depending on the clinical question.
External Auditory Canal
The external auditory canal is easily accessible to direct inspection and so the diagnosis is frequently known prior to imaging. Most imaging is done for staging of congenital anomalies or to identify possible deeper extension of a lesion arising in the canal. Computed tomography is usually the first approach.
Congenital Lesions
Atresia of the external auditory canal is evaluated in axial and coronal planes using a bone algorithm CT. No contrast is used. The thickness of the atretic plate is best appreciated in the coronal plane (Fig. 4.1) (4,5). In a complete atresia the malleus may be fused to the atresia plate. Other fusions and abnormalities of ossicles are often appreciated.
The development of the middle ear and pneumatization of the mastoid are important for surgical planning (6). The width of the middle ear at the oval window and of the air space at the level of the horizontal semicircular canal give a good estimation of the development of the middle ear and can be appreciated in either axial or coronal plane. When atresia of the external auditory canal is associated with a severely atretic middle ear, bone is seen abutting the horizontal canal without an aerated antrum or mastoid (Fig. 4.2). The status of the stapes is assessed on axial and coronal images. The presence and integrity of the oval and round windows is assessed.
In patients with atresia of the external auditory canal the facial nerve usually is in an abnormal location. The mastoid segment appears to “migrate” anteriorly into the location usually taken by the external auditory canal. This is appreciated on either axial or coronal CT. Normally the mastoid segment of the facial nerve canal is located posteriorly in the same coronal plane as the posterior semicircular canal. In atresia of the external auditory canal, that segment of the canal is seen more anteriorly in the same plane as the round window niche. This finding is almost always present with significant atresias. The tympanic segment of the nerve can also be aberrant. The nerve can migrate inferiorly to be positioned
in or near the oval window or even over the promontory (see Facial Nerve section in this chapter).
in or near the oval window or even over the promontory (see Facial Nerve section in this chapter).
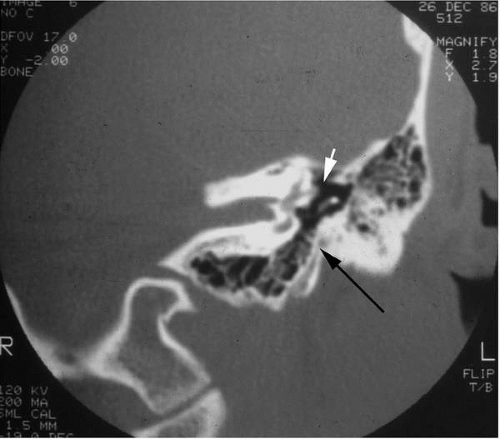 FIG. 4.1 External auditory canal atresia, coronal CT. There is a relatively thick atretic plate (black arrow). The width of the air space at the level of the horizontal semicircular canal (white arrow) is normal. This plane is taken through the level of the oval window. |
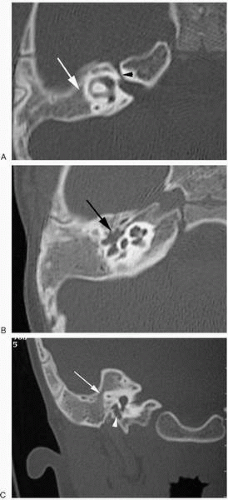 FIG. 4.2 Severe external auditory canal atresia, CT. A: Axial image through the level of the horizontal semicircular canal. There is no development of the mastoid or upper middle ear. Bone (white arrow) abuts the cortex of the otic capsule at the level of the horizontal canal. No air space is visualized. Labyrinthine segment of the facial nerve canal (black arrowhead). B: Axial image of lower middle ear. The middle ear space (arrow) is narrow and opacified. C: Coronal image through the level of the round window. Bone (arrow) is seen immediately adjacent to the horizontal canal. There is a very small middle ear space (arrowhead). |
Finally the status of the labyrinth is documented. Though uncommon, an inner ear anomaly should be excluded to the extent possible by imaging.
Mass Lesions and Infection
Other than atresias, most lesions of the ear are evaluated in a similar way. The location and extent of the lesion are of primary concern. For example, does the lesion extend into the mastoid or through the tympanic membrane into the middle ear (Fig. 4.3)? Is there extension inferior or anterior to the external auditory canal (Fig. 4.4)? Does a lesion extend into the temporomandibular joint or the parotid gland?
Smooth expansion with an intact cortex is seen in keratosis obturans or cholesteatoma. The cortex of the external auditory canal is rounded but not infiltrated or destroyed. There is no deep invasion of the contiguous tissues without coexistent additional infection.
Exostoses produce cortical thickening protruding into and narrowing the canal. Often, centrifugal expansion will involve several walls of the canal. An osteoma tends to have a smaller attachment, presenting more commonly as a single mass. In each case the radiologist documents the proximity to the attachment of the tympanic membrane (Fig. 4.3). Is there a clear area of normal bone separating the lesion from the tympanic annulus?
Carcinoma of the external auditory canal and malignant or necrotizing otitis externa share many findings on imaging and may be evaluated with CT or MRI. Computed tomography has the advantage of showing subtle erosion of cortical bone because these pathologies destroy the cortex of the external auditory canal. There is enough fat in the parotid
gland and along the underside of the external auditory canal that CT is very effective in determining extension into the contiguous soft tissues (Fig. 4.4). Invasion through the cortex of bone or tympanic membrane into the middle ear is seen as obliteration of the air space on CT or as signal where there should be none on MRI. In MRI, both malignant or necrotizing otitis externa and carcinoma tend to be darker on T2 than fluid caused by inflammation or obstruction in the mastoid. Magnetic resonance imaging may more easily define the margin of the pathology within the air spaces. The enhancement of tumors also may be slightly different. Inflamed mucosa tends to enhance slightly more than tumor or malignant or necrotizing otitis externa.
gland and along the underside of the external auditory canal that CT is very effective in determining extension into the contiguous soft tissues (Fig. 4.4). Invasion through the cortex of bone or tympanic membrane into the middle ear is seen as obliteration of the air space on CT or as signal where there should be none on MRI. In MRI, both malignant or necrotizing otitis externa and carcinoma tend to be darker on T2 than fluid caused by inflammation or obstruction in the mastoid. Magnetic resonance imaging may more easily define the margin of the pathology within the air spaces. The enhancement of tumors also may be slightly different. Inflamed mucosa tends to enhance slightly more than tumor or malignant or necrotizing otitis externa.
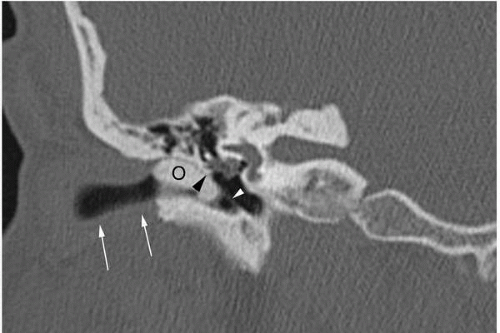 FIG. 4.3 Osteoma of the external auditory canal, coronal CT. The osteoma (O) fills much of the medial external auditory canal. It does not extend beyond the tympanic membrane (white arrowhead) into the middle ear. Note its relationship to the scutum (black arrowhead). The cartilaginous portion of the external auditory canal (white arrows) is faintly visualized on this bone algorithm. The cortex of the osseous external auditory canal is intact. |
Malignant or necrotizing otitis externa tends to pass inferiorly through the fissures of Santorini between the bony and cartilaginous segments of the external auditory canal. This area is well seen in the coronal plane (Fig. 4.4). If there is invasion at this point, the lesion can extend medially, invading the fat in the stylomastoid foramen and extending across the soft tissues beneath the skull base. This may be detected with CT or MRI (7,8). The lesion can invade into the skull base at the petroclival synchondrosis, eventually extending intracranially. This extension is much less common with the advent of newer, more effective antibiotics.
Computed tomography shows the invasion of the cortex of the external auditory canal and extension into the mastoid as well as early extension into the subcranial soft tissues. When a lesion traverses the mastoid or invades other parts of the skull base, MRI is preferred for showing involvement of the dura or the brain. Magnetic resonance imaging is also more sensitive for invasion of muscular structures such as the retropharyngeal or masticator muscles. One must analyze the margin of the tumor to determine if an additional examination is necessary. For instance, if the lesion is first evaluated with CT and is separated from muscle and from dura by intact fat or bone, MRI adds little to the evaluation.
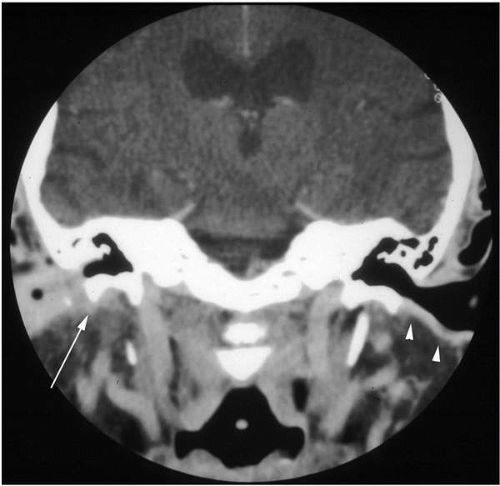 FIG. 4.4 Possible early malignant external otitis, coronal CT soft tissue algorithm. There is thickening of the cartilaginous external auditory canal on the right. A small amount of tissue (arrow) extends into the fatty tissue just beneath the external auditory canal. This is the approximate position of the fissures of Santorini at the junction of the cartilaginous and bony external canal. Compare with the intact fat and parotid just beneath the cartilaginous portion of the external canal (arrowheads) on the left side. |
Middle Ear
The middle ear is evaluated primarily with CT. The key landmarks are small cortical bony structures, ideal for CT imaging.
Chronic Otitis Media and Cholesteatoma
The most common indication for imaging in the middle ear is assessment of chronic otitis media and possible cholesteatoma. Opacification or fluid in the middle ear is obvious on either CT or MR. The advantage of CT is that subtle erosion of bone can be detected and the ossicles can be visualized. Cholesteatoma will erode the lateral wall of the attic and the scutum (junction of lateral wall of the attic and the roof of the external auditory canal), and this may be the earliest finding suggesting the presence of such a lesion (Fig. 4.5). The ossicles may be eroded or displaced. However, the findings may also occur in chronic granulomatous otitis media and are not specific for cholesteatoma.
Often the cholesteatoma has already been diagnosed otoscopically. Indeed, even when the diagnosis has not been confirmed, the most important goal of CT is not necessarily to make the diagnosis but rather to define abnormalities that may lead to complications during surgery. Three major landmarks are critical: the horizontal semicircular canal, the tegmen, and the canal of the facial nerve (Fig. 4.5). Each of these landmarks is represented by a cortical bony wall.
The horizontal semicircular canal protrudes into the antrum. As a cholesteatoma enlarges in the antrum, the lateral bony wall of the horizontal semicircular canal may be eroded (Fig. 4.6). This can be appreciated in axial or coronal imaging as a small lucent defect in the bone. An axial image is taken at an angle to show the entire circumference of the horizontal semicircular canal. The integrity of the bone on this image is very reassuring. Other semicircular canals can be eroded as well, but the horizontal semicircular canal is most commonly involved.
The tegmen tympani may be eroded or displaced by cholesteatoma. Search for a defect or dehiscence is particularly important in postoperative cases. An erosion or surgical defect may result in herniation of dura or even temporal lobe. Unfortunately, the tegmen presents a significant problem for imaging. The bone may normally be thin and lies in a sloping plane at an angle to both standard coronal and axial imaging. Pseudodefects are common because of partial
volume artifact (Fig. 4.5). Because the bone is thinner than the voxel (smallest digital imaging volume), the voxel contains both thin bone and soft tissue. The high density of the bone is averaged with the lower density of the adjacent soft tissue. Because only high densities are displayed as white, the averaged value gives the appearance of soft tissue and thus the bone is not apparent. A very small defect can theoretically be missed. Computed tomography demonstration of a thick intact bone, on the other hand, is a reliable finding. In questionable cases, MRI may be helpful. Magnetic resonance imaging will not show the bone but can show the inferior surface of the temporal lobe and document that there is no herniation of brain into the defect.
volume artifact (Fig. 4.5). Because the bone is thinner than the voxel (smallest digital imaging volume), the voxel contains both thin bone and soft tissue. The high density of the bone is averaged with the lower density of the adjacent soft tissue. Because only high densities are displayed as white, the averaged value gives the appearance of soft tissue and thus the bone is not apparent. A very small defect can theoretically be missed. Computed tomography demonstration of a thick intact bone, on the other hand, is a reliable finding. In questionable cases, MRI may be helpful. Magnetic resonance imaging will not show the bone but can show the inferior surface of the temporal lobe and document that there is no herniation of brain into the defect.
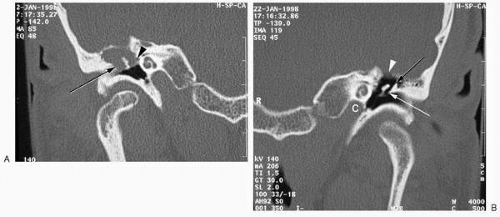 FIG. 4.5 Cholesteatoma of the attic and antrum. A: Coronal CT shows the cholesteatoma opacifying the attic and extending into the antrum. There is erosion of the scutum (arrow). Note the relationship of the lesion to the tympanic segment of the facial nerve canal (arrowhead). B: Coronal CT, opposite, normal side. The middle ear is well aerated and the bony landmarks intact. Note that the tegmen (white arrowhead) is very indistinct due to partial volume artifact. Scutum (white arrow), upper spur of the lateral wall of the attic (black arrow), and carotid canal (C) are also shown. |
The position of the facial nerve and integrity of the fallopian canal are documented. One may not actually see the complete bone covering of the canal. There are common natural dehiscences and, again, partial volume plays a significant role. Erosion by cholesteatoma is unusual, but the radiologist should document the presence of disease adjacent to the canal of the facial nerve.
Finally, imaging can assess the pneumatization of the mastoid and involvement of small recesses of the middle ear, such as the round window niche and the sinus tympani, thus providing to the surgeon details to plan a surgical approach.
Vascular Lesions of the Middle Ear (Red Mass)
At our institution, CT is also the preferred imaging modality when a “red mass” is seen through the tympanic membrane (9). Though MRI can give significant information and can often help make the diagnosis, many radiologists feel that CT provides additional information that can make the initial diagnosis more reliable (10,11). Magnetic resonance imaging or angiography may be done once the initial diagnosis is made.
There are two important landmarks: the lateral bony plate of the carotid canal and the lateral bony plate of the jugular foramen (Fig. 4.7). The position and appearance of these two structures allow the differentiation of the aberrant carotid artery, glomus tympanicum, and glomus jugulare tumors.
The first step in evaluation of the “red mass” is to exclude an aberrant carotid artery. The key landmark is the white line representing the lateral bony wall of the carotid canal. This bony plate is normally just anterior to the cochlea and should be intact. An aberrant artery extends further laterally in the middle ear (Fig. 4.8). The bony wall is usually incomplete, and the vessel is visible along the curve of the promontory of the cochlea. Often a persistent stapedial artery accompanies the aberrant carotid. The foramen spinosum will be absent because the middle meningeal artery arises from the aberrant carotid artery. On MRI an aberrant carotid is recognized by the lateral bend seen as the vessel enters the middle ear. This can also be diagnosed by the characteristic configuration on arteriography, using the frontal projection.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


