The parapharyngeal space (PPS) is a space in the suprahyoid neck that contains fat and is surrounded by several other spaces defined by the fascial layers of the neck. This article presents the spatial anatomy of the PPS and describes the displacement patterns of the PPS fat that are essential for accurate diagnosis and appropriate treatment of pathology arising in this region.
The parapharyngeal space (PPS) is a fascial space of the suprahyoid neck that largely contains fat and is surrounded by several other important fascial spaces. Surgeons may be familiar with the older nomenclature of the “prestyloid” and “post-styloid” parapharyngeal spaces. The post-styloid compartment of the PPS is now designated as the carotid space, whereas the prestyloid compartment is now considered the true PPS. The presence of fat in the PPS allows the radiologist to identify displacement patterns of the PPS and to use a logical algorithm in identifying the anatomic origin of tumors in this region. A clear understanding of spatial anatomy is essential for accurate diagnosis and appropriate treatment of pathology arising from this region. This article covers the basic anatomy of the PPS and surrounding spaces to describe the spatial approach to the differential diagnosis of lesions in this area. Other spaces in the suprahyoid neck, including the retropharyngeal space, the perivertebral space, and the posterior cervical space, are not discussed. Boxes and figures are used to list and illustrate some common conditions in the differential diagnosis pertaining to each space but the reader is referred elsewhere for a more detailed discussion of pathology .
Spatial approach to differential diagnosis
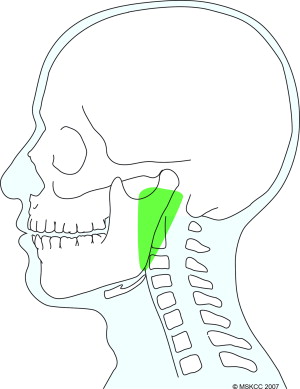
The PPS is an inverted cone-shaped space that extends from the skull base to the level of the hyoid bone on either side of the pharynx ( Fig. 1 ). The anatomic boundaries of the PPS are listed in Box 1 . The PPS is surrounded by other spaces that are bound by the superficial (investing), middle (buccopharyngeal), and deep (prevertebral) layers of the deep cervical fascia. The reader is referred to other sources for detailed anatomy of the facial layers .
Superior
Temporal bone lateral to the attachment of the pharyngobasilar fascia and medial to the foramen ovale and foramen spinosum. Note that none of the skull base foramina are included within the boundaries of the PPS.
Inferior
The greater cornu of the hyoid bone and the posterior belly of the digastric muscle. The PPS blends into the posterior aspect of the submandibular space at this level.
Medial
The buccopharyngeal fascia that covers the pharyngobasilar fascia and constrictor muscles.
Lateral
The fascia overlying the pterygoid muscles and the sphenomandibular ligament. The parotid space communicates with the PPS laterally through the stylomandibular tunnel. This tunnel is enclosed by the stylomandibular ligament which extends from the styloid process to the angle of the mandible, the ascending ramus, and the skull base.
Anterior
The pterygomandibular raphe that extends from the hamulus of the medial pterygoid plate to the posterior aspect of the mylohyoid line on the lingual surface of the mandible.
Posterior
The tensor-vascular-styloid fascia overlying the tensor veli palatini muscle from the medial pterygoid plate to the styloid process.
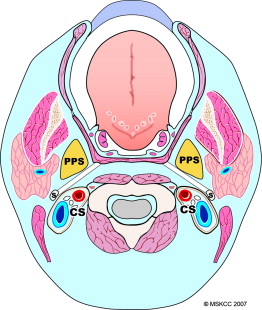
An understanding of the fascial anatomy and spaces of the neck allows a logical approach to differential diagnosis of lesions arising from the PPS or surrounding spaces. The carotid space is actually the designation given to the previously named post-styloid space and is separated from the prestyloid space, or PPS, by the tensor-vascular-styloid fascia overlying the tensor veli palatini muscle ( Fig. 2 ). Unlike squamous cell carcinoma (SCC) that is locally infiltrative and tends to spread across fascial boundaries in the neck, other tumors tend to be limited in local extent by fascial compartments.
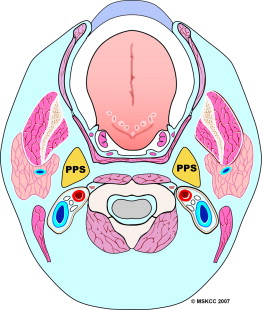
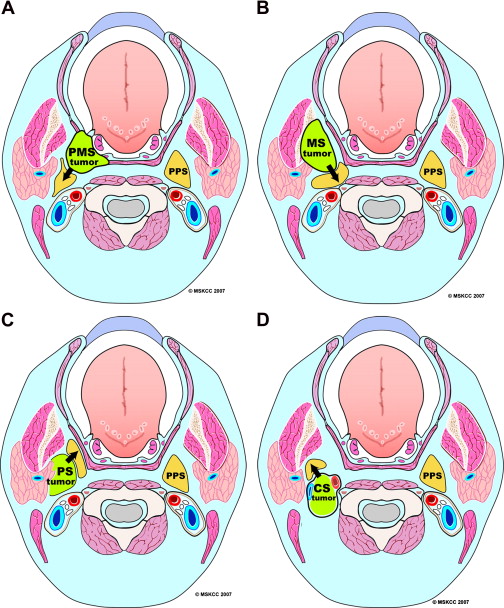
The PPS is centrally located in relation to surrounding spaces that are enclosed by the layers of the deep cervical fascia ( Fig. 3 ). The PPS is a relatively rare site of primary pathology but its significance is that it predominantly contains fat and therefore has a distinct appearance on CT and MRI. The displacement pattern of the PPS fat is an excellent indicator of the possible space of origin of a lesion ( Fig. 4 ) and helps limit the differential diagnosis based on the contents of that space. For example, a tumor arising from the deep lobe of the parotid gland grows medially and thus displaces the adjacent PPS fat anteromedially (see Fig. 4 C). The displacement patterns typical of each space along with some common lesions are described under separate sections.
The pharyngeal mucosal space
The pharyngeal mucosal space (PMS) is the nasopharyngeal and oropharyngeal mucosal lining on the luminal side of the middle layer of the deep cervical fascia. It is lined on the outside by the pharyngeal constrictor muscles and on the inside by squamous mucosa. The space contains minor salivary glands and lymphoid tissue of the Waldeyer ring. Since the PMS is lined by squamous mucosa, squamous cell carcinoma (SCC) is the most common tumor but other tumors, such as minor salivary gland tumors, lymphoma ( Fig. 5 ), and sarcoma, can also occur.
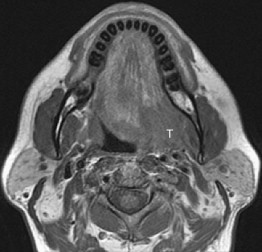
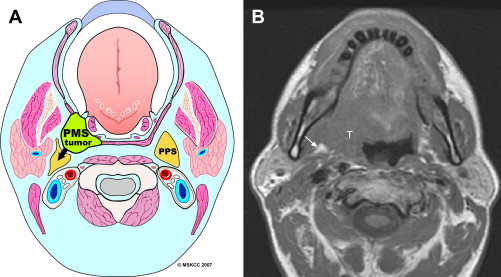
Tumors of the PMS are based on the mucosa or wall of the space with no clear delineating plane between it and the tumor. They may infiltrate the PPS diffusely and replace it ( Fig. 6 ). Alternatively, with benign or less aggressive tumors the PPS fat is displaced posteriorly and laterally ( Fig. 7 ).
The pharyngeal mucosal space
The pharyngeal mucosal space (PMS) is the nasopharyngeal and oropharyngeal mucosal lining on the luminal side of the middle layer of the deep cervical fascia. It is lined on the outside by the pharyngeal constrictor muscles and on the inside by squamous mucosa. The space contains minor salivary glands and lymphoid tissue of the Waldeyer ring. Since the PMS is lined by squamous mucosa, squamous cell carcinoma (SCC) is the most common tumor but other tumors, such as minor salivary gland tumors, lymphoma ( Fig. 5 ), and sarcoma, can also occur.
Tumors of the PMS are based on the mucosa or wall of the space with no clear delineating plane between it and the tumor. They may infiltrate the PPS diffusely and replace it ( Fig. 6 ). Alternatively, with benign or less aggressive tumors the PPS fat is displaced posteriorly and laterally ( Fig. 7 ).
The masticator space
The masticator space (MS) is enclosed by the split layers of the superficial layer of the deep cervical fascia and extends from the skull base to the inferior border of the mandible. It contains the ascending ramus, the posterior body of the mandible, and the muscles of mastication (masseter, medial and lateral pterygoids, and temporalis), the motor and sensory branches of mandibular branch of the trigeminal nerve (V3), and the inferior alveolar artery and vein. The MS extends superolaterally along the lateral surface of the temporalis muscle, divided by the zygoma into supra and infrazygomatic portions ( Fig. 8 ). Anteriorly it is continuous with the buccal space where there is no discrete fascial boundary so that disease processes have free access from one space to the other.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


