Preoperative imaging studies have an important role in facilitating successful localization of adenomas for surgeons. Their use has increased and parallels the recent growth of minimally invasive parathyroidectomy. Based on findings that scintigraphy is reported to have the highest accuracy for localization of adenomas when compared with anatomic imaging techniques, this article discusses the current role and limitations of imaging, with a focus on scintigraphy, in the evaluation of patients before surgery for hyperparathyroidism.
Parathyroidectomy is the treatment of choice for patients with primary hyperparathyroidism and may be indicated in patients with secondary or tertiary hyperparathyroidism if they do not respond to medical therapy. Preoperative imaging studies have an important role in facilitating successful localization of adenomas for surgeons. Their use has increased and parallels the recent growth of minimally invasive parathyroidectomy.
A variety of anatomic and functional imaging techniques can be used to localize parathyroid adenomas, including ultrasound, MRI, CT, and scintigraphy (nuclear medicine). Surgeons may rely on one or a combination of modalities for planning an operation. In many studies, scintigraphy is reported to have the highest accuracy for localization of adenomas when compared with anatomic imaging techniques. This article discusses the current role and limitations of imaging, with a focus on scintigraphy, in the evaluation of patients before surgery for hyperparathyroidism.
Scintigraphy with single-photon emitters
Parathyroid scintigraphy can be accomplished with several different radiopharmaceuticals and techniques. Selenium-75–methionine, an amino acid analog of methionine, and thallium-201/technetium-99m ( 99m Tc)–pertechnetate subtraction imaging are of historical interest and were abandoned because of poor image quality and technical limitations that led to suboptimal accuracy. 99m Tc-sestamibi is the current radiotracer of choice for parathyroid scintigraphy.
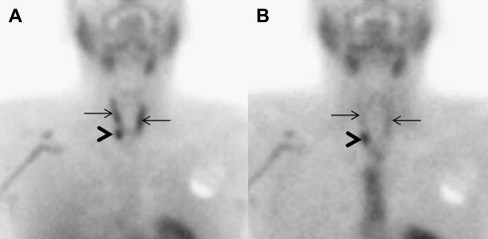
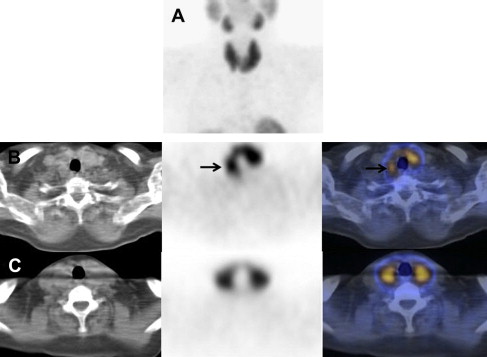
99m Tc-sestamibi is a lipophilic cation that is ultimately sequestered in mitochondria because of transmembrane electrical gradients in the cell and mitochondria. Accumulation of 99m Tc-sestamibi is probably related to increased vascularity and a higher number of mitochondria-rich oxyphil cells in adenomas. Slower release of the tracer from adenomas compared with normal surrounding tissues (parathyroid and thyroid) allows for distinction between the two by imaging ( Fig. 1 ).
The sensitivity of 99m Tc-sestamibi parathyroid scintigraphy for detecting and localizing a single adenoma in patients with primary hyperparathyroidism ranges from 54% to 96%. Few of the studies reported specificity with ranges from 83% to 99%. A meta-analysis, including 20,225 patients with primary hyperparathyroidism, reported an overall 88% sensitivity for detecting a solitary adenoma. Sensitivities were lower for detecting double adenomas (30%) or parathyroid hyperplasia (45%). In patients with tertiary hyperparathyroidism, 99m Tc-sestamibi parathyroid scintigraphy performs well with a sensitivity of approximately 76%.
Various imaging techniques can be used for 99m Tc-sestamibi parathyroid scintigraphy and this is the likely reason for its wide range of diagnostic performance in the literature. Imaging can be performed at 1or 2 time points after radiotracer injection (single- vs dual-phase imaging) and using 2-D planar versus 3-D single-photon emission computed tomography (SPECT) imaging techniques. Specific protocols are determined in part by the nuclear medicine cameras available at an imaging center.
A few studies have directly compared planar with SPECT imaging for detection of parathyroid adenomas. These studies have demonstrated a higher sensitivity of SPECT for detecting and localizing parathyroid adenomas compared with planar imaging. The false-negative rate is reported to be lower for SPECT, and SPECT detects small parathyroid adenomas immediately posterior to the thyroid gland better than planar imaging.
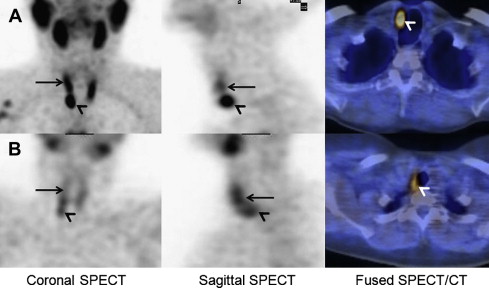
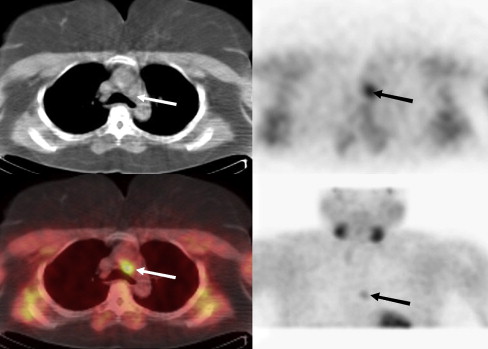
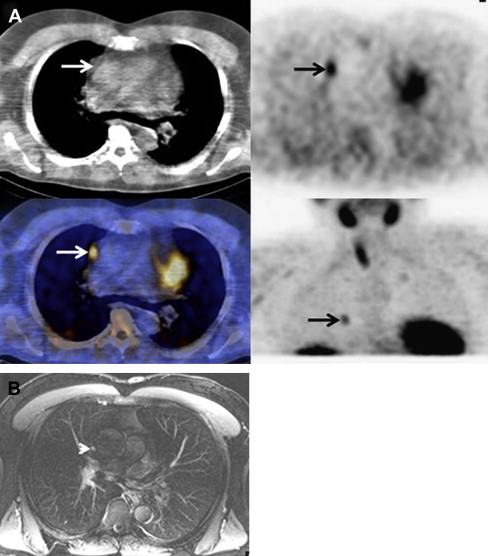
Hybrid SPECT/CT imaging has been a recent focus and studies have demonstrated an advantage of this technique over conventional ones for localization of adenomas, especially in patients with ectopic glands. SPECT/CT allows visualization of corresponding anatomy for differentiation of thyroidal from nonthyroidal tissue and the relationship of the adenoma to adjacent structures ( Fig. 2 ). Mediastinal and intrathyroidal adenomas can be precisely localized, all aiding in the surgical approach ( Fig. 3 ). The precise localization is important because ectopic adenomas can be located in the paraesophageal region (28%), mediastinum (26%), intrathymic region (24%), intrathyroidal region (11%), carotid sheath region (9%), and high cervical positions (2%). The accuracy of adenoma localization may continue to improve as CT components with higher resolution are incorporated into SPECT/CT cameras.
Another consideration in protocol design is single-phase versus dual-phase imaging. Higher sensitivities are reported for dual-phase imaging protocols. The advantage of the dual-phase technique is 2-fold: (1) distinction between abnormal parathyroid tissue and normal parathyroid or thyroid tissue by differential washout between early and late images and (2) localization of a focus of uptake in relation to thyroid tissue on early images. Dual-phase images may also help identify adenomas with very fast washout rates that might be missed on delayed imaging alone.
Lavely and colleagues performed a comprehensive study of 99m Tc-sestamibi parathyroid scintigraphy in 110 patients with primary hyperparathyroidism and no prior neck surgery. Patients underwent planar and SPECT/CT imaging at 15 minutes and 2 hours after injection of 99m Tc-sestamibi. Early and delayed planar, SPECT, and SPECT/CT images were evaluated individually for each patient. Paired image sets (eg, early and delayed planar and early planar and delayed SPECT) were also evaluated. A total of 19 different combinations of imaging technique was evaluated for each patient. Early SPECT/CT with any delayed imaging emerged as the best methodology for preoperative parathyroid adenoma localization (sensitivity approximately 73%, specificity approximately 99%, accuracy approximately 86%, positive predictive value 86%–91%, and negative predictive value approximately 98%). In the absence of SPECT/CT, dual-phase studies with planar or SPECT imaging was the second best technique (sensitivity approximately 58%–66%, specificity approximately 98%, accuracy approximately 78%–82%, positive predictive value approximately 80%–83%, and negative predictive value approximately 97%).
More recent studies have also confirmed the benefit of hybrid SPECT/CT imaging. Neumann and colleagues compared dual isotope iodine-123 ( 123 I)/ 99m Tc-sestamibi SPECT with SPECT/CT. In the patients with primary hyperparathyroidism, the sensitivity (approximately 70%) for localizing an adenoma was not improved with SPECT/CT; however, anatomic localization significantly improved specificity (96% for SPECT/CT vs 48% for SPECT alone, P <.006). In a study of 23 patients, hybrid SPECT/CT accurately localized an adenoma within 19 mm of its intraoperative location in 95% of cases. In addition, the median time from skin incision to adenoma localization was 14 minutes for single adenomas.
Other techniques to optimize preoperative localization of parathyroid adenomas continue to be investigated in the absence of SPECT/CT. Pinhole imaging, which provides a magnified image, has better diagnostic performance versus parallel-hole collimator imaging and SPECT. Pinhole SPECT is also being investigated and early results are encouraging.
Parathyroid scintigraphy with 99m Tc-tetrofosmin, a tracer similar to 99m Tc-sestamibi, has been investigated. Comparisons of the diagnostic accuracy of the two 99m Tc-labeled agents have yielded mixed results. Several studies have shown that 99m Tc-tetrofosmin performs at least as well as 99m Tc-sestamibi, but others have found discordant results with 99m Tc-sestamibi performing better. Nearly all studies have shown that the differential washout of 99m Tc-tetrofosmin from the thyroid gland is slower than that of 99m Tc-sestamibi, resulting in lower adenoma to thyroid/background ratios. For this reason, 99m Tc-sestamibi has remained the radiopharmaceutical of choice in most nuclear medicine imaging centers.
Limitations of Scintigraphy
The most common cause for a false-positive 99m Tc-sestamibi study is accumulation of the tracer in thyroid adenomas ( Fig. 4 ). Other causes of false-positive results are thyroid carcinoma, inflammatory thyroid disease (such as chronic lymphocytic thyroiditis [ Fig. 5 ]), and inflammatory or malignant cervical lymphadenopathy. Subtraction imaging with a thyroid imaging agent in combination with 99m Tc-sestamibi or hybrid SPECT/CT can reduce false-positive results. In the subtraction technique, images with agents that concentrate solely in the thyroid gland (for example, 99m Tc-pertechnetate and 123 I) are subtracted from those obtained with 99m Tc-sestamibi (which accumulates in thyroid tissue and parathyroid adenomas). The resulting subtraction image can then localize the parathyroid adenoma. A major limitation of the subtraction technique is potential artifact generated on the digitally subtracted images due to patient motion during image acquisition.
Some investigators have tried to identify factors that may affect the sensitivity of scintigraphy for detecting a parathyroid adenoma. Scintigraphy has a better sensitivity for detecting large-sized adenomas and single-gland disease. Higher preoperative parathyroid hormone and calcium levels and decreased vitamin D levels are associated with improved sensitivity in some studies. In addition, thyroid suppression has been associated with increased sensitivity for detecting adenomas, whereas decreased sensitivity has been reported with the use of calcium channel blockers, high P-glycoprotein levels, and multidrug resistance proteins. The cohorts investigated in the various studies, however, were fairly specific and the results cannot be generalized to all patients undergoing 99m Tc-sestamibi scintigraphy.
Given the various techniques available for performing parathyroid scintigraphy, it is important for referring physicians to be aware of the imaging technique used for their individual patients as it may have impact on the diagnostic performance of the test. Collaboration between surgeons and nuclear medicine physicians/radiologists may also help to improve the accuracy of gland localization.
Recurrent Primary Hyperparathyroidism
A persistently elevated parathyroid hormone level after curative therapy may be due to progression of underlying disease after response to bone mineralization or initial surgery failure. Failure to recognize and adequately resect multigland disease at initial surgery is one of the most common causes for failed initial surgery. This remains a challenge because detection of multigland disease is a limitation of 99m Tc-sestamibi parathyroid scintigraphy.
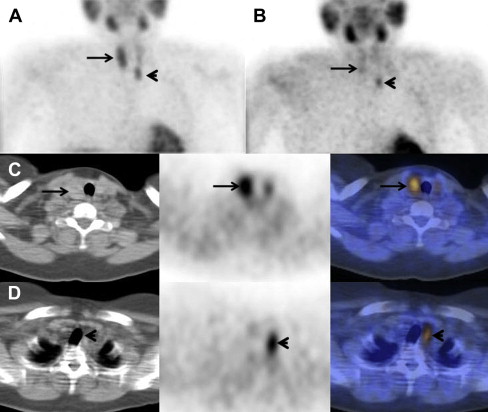
Another significant cause of failed initial surgery is lack of detection of an ectopically located gland ( Fig. 6 ). The frequency of multiple or ectopic glands, often coexisting, as the cause for recurrence ranges from 44% to 70%. In one study, 99m Tc-sestamibi parathyroid imaging was reported to have a sensitivity of 65% for localizing these recurrences. Jaskowiak and colleagues reported that the most common site of a missed ectopic adenoma is the tracheoesophageal grove ( Fig. 7 ). Lavely and colleagues reported that the advantage of combined SPECT/CT seems to be its ability to differentiate ectopic superior glands in the tracheoesophageal groove (located inferior and posterior to the thyroid gland) from true inferior glands (see Fig. 2 ). Wider use of this technique in the future may prove to decrease recurrence rates due to failed initial surgeries.

Patients with a prior history of thyroid or parathyroid surgery were included in several studies evaluating parathyroid scintigraphy and the technique seems equally sensitive for localizing and detecting parathyroid adenomas regardless of the surgical status of the neck. Civelek and colleagues reported sensitivities of 87% versus 92% for delayed 99m Tc-sestamibi SPECT imaging in those with (N = 51) versus without (N = 287) a prior history of neck surgery. Similarly, Billotey and colleagues reported 91% overall sensitivity for adenoma detection in all patients and 87% sensitivity for 39 patients undergoing reoperation. In the reoperative setting, 99m Tc-sestamibi parathyroid imaging was superior to anatomic imaging modalities.
In 3% of cases, persistent or recurrent hyperparathyroidism may be due to regrowth of previously resected tumor or remnant tissue. Additionally, when surgery for secondary or tertiary hyperparathyroidism is performed, one-half of a gland is often reimplanted into a graft site and recurrence can occur due to hyperfunctional activity within the reimplanted parathyroid tissue. In these cases, it is imperative for an imaging physician to know the location of the reimplanted tissue so directed imaging can be performed. When patients with secondary hyperparathyroidism recur, 99m Tc-sestamibi imaging is useful to determine if the failure is due to a hyperfunctioning graft or an ectopic fifth gland, necessitating a change in management. Itoh and Ishizuka confirmed the high sensitivity (100% in this study) of 99m Tc-sestamibi for the preoperative localization of hyperfunctioning parathyroid glands in patients with persistent or recurrent hyperparathyroidism after 4-gland parathyroidectomy with autoimplantation of parathyroid tissue.
Radioguided parathyroidectomy
Radioguided parathyroidectomy is a technique that involves the injection of 99m Tc-sestamibi before surgery and intraoperative use of a gamma probe that can help localize the parathyroid adenoma for the surgeon. Several approaches to radioguided parathyroidectomy are reported. Some groups administer the radiotracer, obtain imaging studies, and then perform surgery within a 2- to 3-hour time frame on the same day whereas others omit the imaging on the day of surgery and inject the tracer before the start of the operation and only use the gamma probe intraoperatively. For both approaches, localization of the adenoma is performed by scintigraphy or other imaging modalities before surgery. A small amount of radioactivity is required when using the gamma probe as compared with imaging studies; therefore, an advantage of not obtaining images on the day of surgery is that the surgical team is exposed to less radiation. Another advantage is that the shorter time interval between tracer injection and surgery may enhance a surgeon’s ability to detect those adenomas that have rapid washout of radiotracer.
The operative technique for using the gamma probe is reviewed by Mariani and colleagues. In general, a parathyroid-to-thyroid count ratio of greater than 1.5 is suggestive of a parathyroid adenoma. Once removed, an ex vivo count rate of at least 20% greater than thyroid background (counted in vivo) confirms the resection of an adenoma. The reported accuracy for distinguishing adenoma from multigland hyperplasia was 100% in the initial studies describing the “greater than 20% rule.”
Subsequent studies have shown ex vivo count rates of greater than 20% in thyroid nodules and hyperplasia limiting the application of the initial observation. Rubello and colleagues suggested that an explanation for this might be that the timing between the 99m Tc-sestamibi injection and surgery was longer (2–3 hours) in the initial studies, which allowed for additional washout from nonadenomas. The optimal timing to surgery may vary from patient to patient and a patient-specific, optimal time-to-surgery protocol has been described. Surgery is performed based on the timing of peak adenoma-to-background ratio as determined by dynamic imaging.
The usefulness of radioguided parathyroidectomy in patients with negative preoperative 99m Tc-sestamibi imaging studies is unclear. In 2005, Rubello and colleagues reported that from a surgeon’s perspective, use of the gamma probe was not helpful in 20 patients with negative scans. Forty percent (8/20) of these patients demonstrated multigland disease. More recently, however, Chen and colleagues found equivalent cure rates and major complication rates using radioguided parathyroidectomy in patients with negative (n = 134) versus positive (n = 635) preoperative 99m Tc-sestamibi scans. In the scan-negative group, there was a higher rate of multigland disease and the parathyroid gland weight was lower. Both of these are known to cause false-negative results on scintigraphy. The in vivo and ex vivo count rates were also lower in the scan-negative versus scan-positive patients but significantly greater than background counts in both instances.
Proposed guidelines for radioguided minimally invasive parathyroidectomy include its use for patients with a high probability of a solitary adenoma and a normal thyroid gland. Other considerations are optimizing the preoperative scintigraphy protocols based on all available information, minimizing radiation exposure to the surgical team, and determining the completeness of surgical resection based on in vivo and ex vivo gamma counting data as well as a documented decline in intraoperative parathyroid hormone levels.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


