Imaging Modalities in Ophthalmology
14.1 Plain Films Radiography
Description
Images of radiopaque tissues obtained by exposure of special photographic plates to ionizing radiation.
Uses in Ophthalmology
May be used to identify or exclude radiopaque intraorbital or intraocular foreign bodies. However, computed tomography (CT) is the study of choice to evaluate for foreign bodies, as CT has greater contrast sensitivity over conventional radiography. Plain films remain a valid screening modality before magnetic resonance imaging (MRI) if an occult metallic foreign body is suspected. Plain films should never be used in the setting of trauma or for the diagnosis of orbital fractures.
14.2 Computed Tomography
 Figure 14.2.1 Axial soft tissue window of inferior orbit shows abnormality, which is difficult to assess. |
 Figure 14.2.2 Coronal soft tissue window shows a large blowout fracture of the orbital floor. This finding was missed on the axial study in Figure 14.2.1, demonstrating the importance of reviewing both axial and coronal images. |
Description
CT uses ionizing radiation and computer-assisted formatting to produce multiple cross-sectional planar images. Possible image planes include axial, direct coronal, reformatted coronal, and reformatted parasagittal images. Bone and soft tissue windows should always be reviewed in axial, coronal, and parasagittal orientations (see Figures 14.2.1 to 14.2.3). Orbital studies should be obtained using the lowest radiation dose necessary for diagnosis (As Low As Reasonably Acceptable [ALARA]—SEE BELOW). This is especially important
in children; for accreditation by the American College of Radiology, health care facilities must maintain specific pediatric protocols for CT. Radiopaque iodinated contrast allows for more extensive evaluation of vascular structures and areas where there is a breakdown of the normal capillary endothelial barrier (as in inflammation).
in children; for accreditation by the American College of Radiology, health care facilities must maintain specific pediatric protocols for CT. Radiopaque iodinated contrast allows for more extensive evaluation of vascular structures and areas where there is a breakdown of the normal capillary endothelial barrier (as in inflammation).
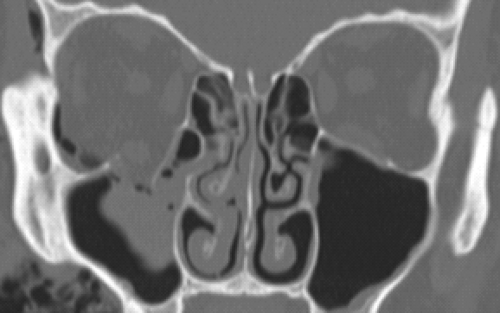 Figure 14.2.3 Coronal bone window shows the fracture again. In bone windows, the soft tissue detail fades, but bone detail is enhanced, allowing for better examination of bony anatomy. |
Uses in Ophthalmology
Excellent for defining bone abnormalities such as fractures (orbital wall or optic canal), calcification, or bony involvement of a soft tissue mass.
Locating suspected intraorbital or intraocular metallic foreign bodies. Glass, wood, and plastic are less radiopaque and therefore more difficult to isolate on CT.
Soft tissue windows are good for determining some pathologic features, including orbital cellulitis/abscess, inflammation, and tumors. May be useful in determining posterior scleral rupture when clinical examination is inconclusive, but B-scan ultrasonography may be more sensitive. CT should never be used to definitively rule out globe rupture; clinical examination and/or surgical exploration are more sensitive modalities.
Excellent for imaging paranasal sinus anatomy and disease.
Head CT is very sensitive for locating parenchymal, subarachnoid, subdural, epidural, and retrobulbar hemorrhage in either acute or subacute settings.
Imaging modality of choice for most cases of thyroid eye disease. SEE 7.2.1, THYROID EYE DISEASE.
Loss of consciousness or unwitnessed head trauma with poor history requires CT of the brain unless otherwise recommended by a neurosurgical consultant. Note that CT of the brain does not provide adequate detail of the orbital anatomy, and orbital CT does not image the entire brain. Each site has its own specific, separate CT protocol.
Guidelines for Ordering an Orbital Study
Always order a dedicated orbital study if ocular or orbital pathology is suspected. Always include views of paranasal sinuses and cavernous sinuses.
Order both direct axial and direct coronal views if older scanners are used. Newer, multidetector (multislice) CT scanners provide excellent views in coronal and parasagittal planes with very short scan times and no patient repositioning. Multidetector CT is preferred when available.
When evaluating traumatic optic neuropathy, request 1-mm cuts of the orbital apex and optic canal to rule out bony impingement of the optic nerve. SEE 3.11, TRAUMATIC OPTIC NEUROPATHY.
When attempting to localize ocular or orbital foreign bodies, order 1-mm cuts.
Intravenous contrast may be necessary for suspected infections or inflammatory conditions. Contrast is helpful in distinguishing orbital cellulitis from abscess. However, it is not mandatory to rule out orbital inflammation or postseptal involvement. Relative contraindications for contrast include renal failure, diabetes, congestive heart failure, multiple myeloma or other proteinemias, sickle cell disease, multiple severe allergies, and asthma. Check renal function and discuss the options with the radiologist for patients in whom renal insufficiency is suspected. Shellfish allergy is not a contraindication for CT contrast.
 NOTE: The radiologist may recommend premedication with corticosteroids and antihistamines if contrast is required and a prior allergy is suspected. Follow the protocol recommended by your radiology department.
NOTE: The radiologist may recommend premedication with corticosteroids and antihistamines if contrast is required and a prior allergy is suspected. Follow the protocol recommended by your radiology department.
Obtain pregnancy test before obtaining CT scans in females of childbearing age.
CT angiography (CTA) is helpful in diagnosing intracranial vascular pathology, including aneurysms. It is available on all multidetector CT scanners and may be more sensitive than magnetic resonance angiography (MRA) in specific clinical situations. However, it requires the use of intravenous iodinated contrast. Also note that CTA requires significantly more radiation than CT. CTA should be avoided if at all possible in children; MRA is the preferred modality in the pediatric age group.
CT scans may be obtained in children with careful consideration of the risk of radiation exposure versus benefits of performing the scan. According to the ALARA paradigm, it is best to avoid CT if possible in children unless there is no reasonable substitute. Check with your radiologist about using a pediatric protocol to limit radiation exposure. Each CT scan exposes children to a cumulative radiation dose that may increase the risk of malignancy over their lifetime. Radiation exposure from CT scans in children is of particular concern when serial imaging is required. In these cases, MRI/MRA is often a better choice for children, although sedation may be needed.
14.3 Magnetic Resonance Imaging
Description
MRI uses a large magnetic field to excite protons of water molecules. The energy given off as the protons re-equilibrate to their normal state is detected by specialized receivers (coils), and that information is reconstructed into a computer image.
Obtains multiplanar images without loss of resolution.
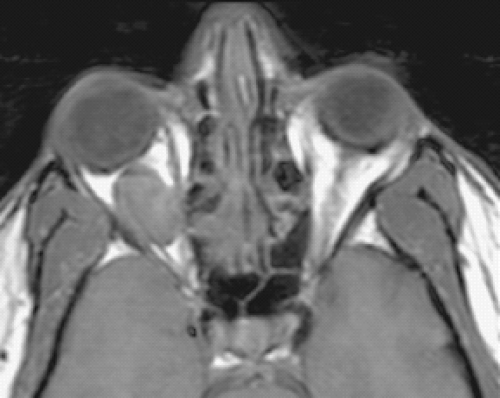
Figure 14.3.1 Axial T-1-weighted image without fat suppression or gadolinium. The vitreous is dark (hypointense) relative to the bright signal from fat. A well-circumscribed mass is clearly visible in the right orbit, also hypointense. Most orbital lesions are dark in T1 prior to gadolinium injection. The notable exceptions are listed in Table 14.3.2.
The basic principles of MRI are listed in Table 14.3.1. Figures 14.3.1 to 14.3.3 provide specific examples.
Contrast studies can be ordered using gadolinium, a well-tolerated, non–iodine-based paramagnetic agent.
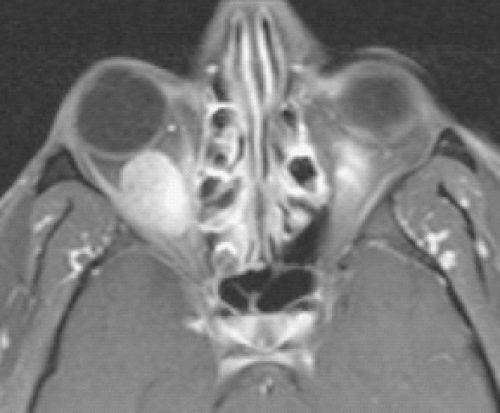
Figure 14.3.2 Axial T-1 image with fat suppression and gadolinium. Note how both the vitreous and fat are dark, but the extraocular muscles become bright. The orbital mass is now clearly visible. This technique should be performed in all orbital MRIs.
Diffusion weighted imaging (DWI) is a technique that measures the Brownian motion of water within tissue. Lesions that are tightly packed by cells with a high nuclear to cytoplasmic ratio will minimize Brownian motion and “restrict diffusion.” DWI is often coupled with
an apparent diffusion coefficient (ADC) image. The use of DWI/ADC in the orbit is limited because of proximity of the CNS but can be useful in certain disorders such as lymphoma.
 Figure 14.3.3 Axial T-2-weighted image. The vitreous is hyperintense (bright) relative to the orbital fat. The lesion is also bright but in some cases may be isointense with the surrounding fat. |
Uses in Ophthalmology
Excellent for defining the extent of orbital/central nervous system masses. Signal-specific properties of certain pathology may be helpful in diagnosis (see Table 14.3.2).
Poor bone definition (e.g., fractures).
Excellent for diagnosing intracranial, cavernous sinus, and orbital apex lesions, many of which affect neuro-ophthalmic pathways.
Gadolinium is essential in defining lesion extent in suspected neurogenic tumors (meningioma, glioma).
Table 14.3.1 Summary of MRI Sequencesa
T1
Fat Suppression
Gadolinium
T2
Properties
Useful for intraorbital structures such as optic nerve, extraocular muscles, and orbital veins. The strong fat signal within the orbit gives poor resolution of lacrimal gland and may also mask intraocular structures.
T1-weighted images with bright intraconal fat signal suppressed in the orbit, allowing for better anatomic detail. Essential for all orbital MRIs.
A paramagnetic agent that distributes in the extracellular space and does not cross the intact blood–brain barrier. Gadolinium is best for T1, fat-suppressed images. The lacrimal gland and extraocular muscles “enhance” with gadolinium. Essential for all orbital MRIs. Always order with fat suppression in orbital studies.
Suboptimal intraocular contrast. Demyelinating lesions (e.g., multiple sclerosis) are bright.
Interpretation
Fat is bright (high signal intensity). Vitreous and intracranial ventricles are dark.
Vitreous and fat are dark. Extraocular muscles are bright after gadolinium is administered.
Most orbital masses are dark on T1 and become bright with gadolinium enhancement. Notable exceptions are listed in Table 14.3.2.
Fluid-containing structures such as vitreous and CSF are bright. Melanin is dark.
The FLAIR sequence on T2 suppresses the bright signal from CSF and is especially helpful in identifying the periventricular lesions of demyelinating disease.
NOTE: In general, conventional “closed” MRI scanners provide better resolution and fat suppression than open scanners, unless the open scanner contains a stronger magnet. As a rule, always try to use conventional “closed” scanners for orbital studies.
a Note: High-flow areas create a dark area, “flow void,” which is helpful in identifying arterial structures (e.g., carotid siphon within the cavernous sinus).
Table 14.3.2 Tissues/Lesions That Appear Bright (Hyperintense) Relative to Vitreous Before Gadolinium Injectiona
Tissues/Lesions
Examples
Fat
Lipoma, liposarcoma
Mucus/proteinaceous material
Dermoid cyst, mucocele, dacryocele, craniopharyngioma
Melanin
Melanoma
Subacute blood (3–14 days old)
Lymphangioma with blood cyst, hemorrhagic choroidal detachment, spontaneous orbital hematoma
Certain fungal infections (iron scavengers)
Aspergillus
a Note: Most orbital lesions will become hyperintense after gadolinium infusion.
All patients with clinical signs or symptoms of optic neuritis from suspected demyelinating disease should undergo brain MRI with gadolinium. Fluid-attenuated inversion recovery (FLAIR) images are especially useful. See Figure 14.3.4 and 10.14, OPTIC NEURITIS.
For orbital studies, fat suppression should always be used in conjunction with intravenous gadolinium to enhance the visualization of the underlying pathology (e.g., optic neuritis, fat-containing lesions). Note that gadolinium without fat suppression may cause pathology to “disappear” into surrounding orbital fat.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


