This article discusses the rationale and indications for image-guided fine needle aspiration and biopsy of a spectrum of head and neck masses, with an emphasis on CT-guided procedures in the suprahyoid neck. Preparation of patients before their appointment in the radiology department, obtaining informed consent, the technique and approaches, and postprocedural care are reviewed.
The significant increase in cross-sectional CT and MRI studies owing to greater availability as well as the expanding clinical indications for the performance of these studies has led to the detection of an increasing number of nonpalpable head and neck masses. Many of these masses are not clinically suspected, are asymptomatic, and are found serendipitously.
Most palpable neck masses are aspirated by the clinical services caring for the patients, including otorhinolaryngologists, endocrinologists, and cytopathologists. Fine needle aspiration (FNA) of palpable lesions is a relatively accurate diagnostic tool in the head and neck, particularly of the salivary glands . Referrals for imaging-guided FNA or biopsy are severalfold. Frequently, masses at the skull base are detected on CT or MRI studies performed for other reasons such as headaches, dizziness, and neck pain. Other indications for imaging guided procedures of the head and neck include:
- •
Inconclusive cytology on FNA performed by palpation in the referring clinician’s office
- •
Deep skull base masses found on ear, nose, and throat patient workups
- •
Palpable masses near critical structures (common or internal carotid arteries, vertebral artery, and cranial nerves, especially the facial and trigeminal nerves)
- •
Discrimination of tumor from treatment changes in necks previously managed with irradiation and/or surgery where physical examination may be uninformative or misleading, even when recurrent tumor is suspected
Image-guided FNA of head and neck lesions is a relatively quick and safe outpatient procedure in experienced hands. Equally important, this procedure improves patient care when used appropriately as many lesions such as metastatic disease and hematologic malignancies are not surgical disease and are usually managed with radiation therapy and/or chemotherapy. Furthermore, certain benign lesions such as paragangliomas or schwannomas may be followed in select patient populations (older patients, patients with poor underlying medical status, poor surgical candidates, or patients electing not to be managed surgically). In other instances, patients may select radiation therapy rather than surgery.
The radiologist’s arsenal
The tools available to the radiologist for performance of head and neck imaging-guided FNA and biopsy include ultrasound (US), CT, and MRI. Sonographic guidance, when possible, is advocated for biopsy of head and neck lesions because of its real-time capability. It is excellent for superficial masses, and should be the diagnostic tool of choice for thyroid nodules and small lateral cervical lymph nodes with suspected pathology owing to architectural abnormalities detected on imaging (such as in the setting of suspected metastatic-differentiated thyroid cancer) . However, lesions at the skull base and those deep to the bony structures and near air-containing spaces are not well visualized during sonography . CT- and MRI-guided FNA can accurately evaluate lesions that are poorly accessible or deeply located in the head and neck. CT guidance has the added advantage of “quick” localization and aspiration time .
MRI-guided FNA has been performed with good results and little morbidity . It provides excellent soft-tissue resolution and has the advantage of the lack of ionizing radiation. Disadvantages of MRI-guided FNA and biopsy include limited availability (particularly with open MRI systems), longer image acquisition and procedural times, and the need for instruments that are compatible with a magnetic field. These factors also increase the cost of using MRI guidance. Although MRI guidance may have an expanded role in the future, especially with open high-field-strength magnets and the evolution of intra-operative MRI units, CT is currently the imaging technique of choice for FNA or biopsy of deep-seated or poorly localized head and neck lesions.
CT guidance has advantages over US in that it has less image degradation related to the air-containing aerodigestive structures and the adjacent bones. Although bony structures may cause some beam-hardening artifact on CT, this has been substantially reduced by thin-section collimation. Other advantages of CT include access to “deep” lesions at the skull base with accurate assessment of critical adjacent anatomy, most notably the arteries. The time that it takes to perform CT-guided interventions is decreasing with the advent of multidector-row CT. In experienced hands, CT-guided FNA in the head and neck is a well-tolerated procedure devoid of notable complications, and it is an effective alternative to the more invasive open surgical biopsy. The discussion that follows focuses on CT-guided FNA procedures. The value of CT-guided FNA includes its relatively low invasiveness, the use of small needles in an area where several vascular and neural structures are present, the lack of an external scar from the procedure, and, equally important, the extremely low complication rate .
Ultrasound-guided fine needle aspiration for thyroid-related disease
Real-time US of the thyroid gland is usually performed with high-resolution linear array transducer ranging from 7.5 to 12 MHz . The patient is placed in a supine position and the neck is mildly hyperextended. The thyroid gland is imaged in its entirety, both in transverse and longitudinal planes. The carotid arteries and jugular veins are posterior and lateral to the thyroid lobes, respectively, and provide excellent anatomic markers during the examination. The examination also includes assessment of the midline neck from the sternal notch to above the hyoid bone. The sonographer should also image the lateral cervical lymph nodes, particularly in the setting of suspected malignancy.
Limitations of sonography include a high degree of operator dependency and the inability of sonography to detect retrotracheal or intrathoracic extension of an enlarged thyroid owing to overlying air or bone. US is also limited in detecting extension of thyroid malignancy into the adjacent trachea, esophagus, or other adjacent soft-tissue structures of the head and neck.
Sonographic guidance, when possible, is advocated for biopsy of head and neck lesions because of its real-time capability. It is excellent for superficial masses, and should be the diagnostic tool of choice for thyroid nodules ( Fig. 1 ). FNA of all palpable nodules in euthyroid patients is the accepted standard of care for assessing the nodule for cancer. In the hands of experienced cytologists, FNA has a high accuracy rate. In many cases, nodules that are palpable undergo biopsy by clinicians without imaging guidance. Sonography is pursued for guidance if the patient has had a prior nondiagnostic biopsy, or if the nodule is known to be complex, as sonography can guide FNA of the solid component and significantly decrease the likelihood of a nondiagnostic aspirate . Even if the patient has had a diagnostic FNA by palpation, sonography of the gland may be indicated to evaluate for nonpalpable coexistent nodules, which may influence management in up to 63% of patients . Specimens may be obtained with 22- to 25-gauge needles. Typically, three separate passes are made to ensure the most adequate specimen possible. Interpretation requires a skilled cytopathologist. Benign nodules may be followed and malignant or suspicious nodules are usually surgically resected. In cases where FNA is nondiagnostic, repeat aspiration in 6 to 8 weeks, or surgical excision may be necessary .
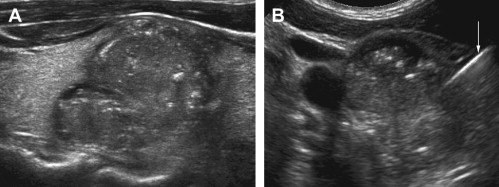
Lateral cervical lymph nodes (including those normal in size) with suspected pathology owing to architectural abnormalities (such as in the setting of suspected metastatic disease in patients with a history of differentiated thyroid cancer) are readily detected on US imaging and are accessible for US-guided FNA ( Fig. 2 ) .

Ultrasound-guided fine needle aspiration for thyroid-related disease
Real-time US of the thyroid gland is usually performed with high-resolution linear array transducer ranging from 7.5 to 12 MHz . The patient is placed in a supine position and the neck is mildly hyperextended. The thyroid gland is imaged in its entirety, both in transverse and longitudinal planes. The carotid arteries and jugular veins are posterior and lateral to the thyroid lobes, respectively, and provide excellent anatomic markers during the examination. The examination also includes assessment of the midline neck from the sternal notch to above the hyoid bone. The sonographer should also image the lateral cervical lymph nodes, particularly in the setting of suspected malignancy.
Limitations of sonography include a high degree of operator dependency and the inability of sonography to detect retrotracheal or intrathoracic extension of an enlarged thyroid owing to overlying air or bone. US is also limited in detecting extension of thyroid malignancy into the adjacent trachea, esophagus, or other adjacent soft-tissue structures of the head and neck.
Sonographic guidance, when possible, is advocated for biopsy of head and neck lesions because of its real-time capability. It is excellent for superficial masses, and should be the diagnostic tool of choice for thyroid nodules ( Fig. 1 ). FNA of all palpable nodules in euthyroid patients is the accepted standard of care for assessing the nodule for cancer. In the hands of experienced cytologists, FNA has a high accuracy rate. In many cases, nodules that are palpable undergo biopsy by clinicians without imaging guidance. Sonography is pursued for guidance if the patient has had a prior nondiagnostic biopsy, or if the nodule is known to be complex, as sonography can guide FNA of the solid component and significantly decrease the likelihood of a nondiagnostic aspirate . Even if the patient has had a diagnostic FNA by palpation, sonography of the gland may be indicated to evaluate for nonpalpable coexistent nodules, which may influence management in up to 63% of patients . Specimens may be obtained with 22- to 25-gauge needles. Typically, three separate passes are made to ensure the most adequate specimen possible. Interpretation requires a skilled cytopathologist. Benign nodules may be followed and malignant or suspicious nodules are usually surgically resected. In cases where FNA is nondiagnostic, repeat aspiration in 6 to 8 weeks, or surgical excision may be necessary .
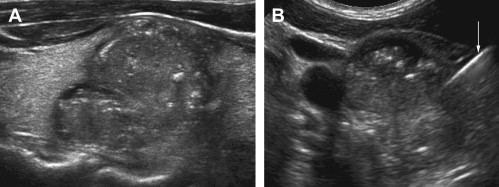
Lateral cervical lymph nodes (including those normal in size) with suspected pathology owing to architectural abnormalities (such as in the setting of suspected metastatic disease in patients with a history of differentiated thyroid cancer) are readily detected on US imaging and are accessible for US-guided FNA ( Fig. 2 ) .
CT-guided procedures of the head and neck
Patient preparation
Preparation of the patient before CT-guided FNA is in general minimal, especially compared with that required for open surgical procedures. First, it is essential that the radiologist performing the procedure review the initial diagnostic CT or MRI scan where the abnormality was detected to be certain that it is feasible to do the procedure. For superficial lesions such as in the superficial parotid gland or the lateral neck, where pressure may be applied following the aspiration to prevent or control any light bleeding, and where intravenous (IV) contrast is not needed, preprocedural blood work is usually not necessary. For deep lesions (usually those in the suprahyoid extramucosal spaces, including the parapharyngeal/deep lobe parotid space, retropharynx, carotid space, prevertebral and masticator spaces), PT, PTT, INR, and platelet count are usually performed. If IV contrast is anticipated to aid in lesion localization and/or to map the carotid or vertebral arteries, a BUN and CR are necessary. Occasionally, additional blood work may be requested in select circumstances such as a suspected paraganglioma (serum catecholamines and 24-hour urine may be indicated). Patients are instructed not to eat for 4 hours before their procedure in the advent that the administration IV contrast may be necessary. This is to prevent aspiration in those occasional cases where patients may experience nausea and vomiting as a reaction to the IV-administered iodinated contrast material.
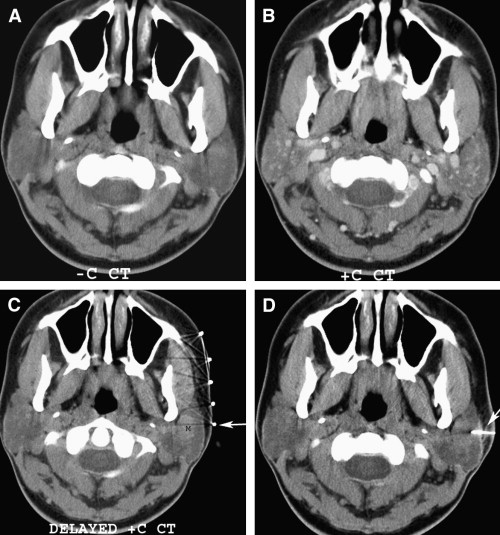
In the majority of cases, IV contrast is not necessary. In the present author’s practice, approximately 7% to 10% of cases get an enhanced CT scan. Frequently, the radiologist is able to use the initial diagnostic CT or MRI study to localize and track critical structures such as the internal carotid artery (ICA) near the mass to be biopsied. However, IV contrast material can be very helpful in mapping out arteries, especially with lesions localized in the carotid and prevertebral/vertebral spaces, or when aspirating deep, high jugular lymph nodes. In addition, contrast-enhanced studies, including delayed imaging, occasionally may help to improve lesion conspicuity. In the author’s practice, this has been particularly true with parotid lesions, especially benign mixed tumors ( Fig. 3 ).
General anesthesia is not required, and more often than not, sedation is not needed. The pain associated with the procedure is usually minimal when adequate local anesthesia is used. In fact, the risk of an adverse reaction to general anesthesia and even sedation is greater than the risk of the procedure itself. The needle used to perform these procedures is frequently smaller than the IV catheter and, not infrequently, needles used for drawing blood samples. Discomfort that may occur during the aspiration usually largely resolves when the needle is removed.
Following the procedure, the patient is observed in the radiology department by the nursing staff for 30 to 60 minutes, and is then discharged home. Discharge instructions are given to the patient before and following the procedure both verbally and in writing. The patient is instructed to take acetaminophen for minor pain that may occur during the first 12 to 24 hours following the procedure, and to call if there is excessive pain, swelling, bruising, elevated temperature above 100.5°F orally (patients are told to take their temperature only if they are not feeling well), or with any other questions or concerns. Usually, patients are allowed to resume their normal diet within 2 hours following their procedure.
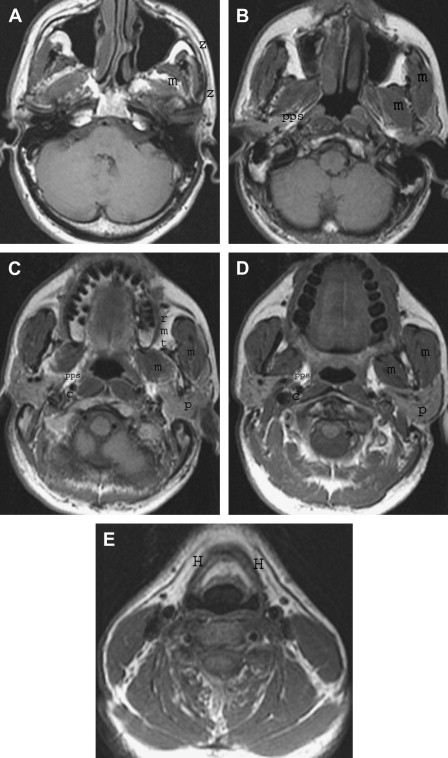
Anatomy
Several approaches for imaging-guided FNA of the head and neck have been described, and approaches are selected based on the anatomic location of the lesion to be biopsied. For masses in the suprahyoid neck and skull base, approaches for FNA include subzygomatic, retromandibular (transparotid), paramaxillary (transfacial), transoral, and posterior. In the infrahyoid neck, lesions are typically approached from an antero-lateral or posterior approach. Thorough knowledge of the cross-sectional anatomy of the neck and skull base ( Fig. 4 ) is essential for planning a safe, quick, and diagnostic imaging-guided procedure, especially in the suprahyoid neck.