Purpose
To assess the extent to which incidence rates calculated for common ocular diseases by using claims data may be overestimated according to the length of the disease-free look-back period used in the analysis.
Design
Retrospective longitudinal cohort analysis.
Methods
Billing records of 2457 persons continuously enrolled for 11 years in a managed-care network were searched for International Classification of Diseases (ICD-9-CM) diagnoses of cataract, open-angle glaucoma (OAG), nonexudative age-related macular degeneration (ARMD), and nonproliferative diabetic retinopathy (NPDR) at eye-care visits in the first half of 2001, the second half of 2010, and 2011. For each condition, incidence rates calculated by using “look-back” periods ranging from 0.5-9 years were compared with best estimates from a gold-standard period of 9.5 years.
Results
With a 1-year disease-free look-back period, incidence was overestimated by 260% for cataract, 135% for OAG, 209% for ARMD, and 300% for NPDR. Expanding the disease-free look-back period to 3 years resulted in a reduction of incidence overestimation to 40% for cataract, 14% for OAG, 45% for ARMD, and 100% for NPDR. A 5-year look-back period yielded incidence rates that were overestimated by <30% for all 4 conditions.
Conclusions
In our claims-data analysis of 4 common ocular conditions, a disease-free interval ≤1 year insufficiently distinguished newly diagnosed from pre-existing disease, resulting in grossly overestimated incidence rates. Using look-back periods of 3-5 years, depending on the specific diagnosis, yielded considerably more accurate estimates of disease incidence.
In recent years a growing number of researchers have relied on data from large health care claims databases to study the epidemiology of diseases and trends in resource use and patient outcomes. Advantages of using large claims databases rather than other data sources include very large sample sizes (allowing the study of uncommon conditions); the ability to follow participants longitudinally, often for many years, to observe associations between exposures (eg, medication use) and outcomes; the absence of reporting bias; improved accuracy, compared with patient self-report, on the types of medical conditions diagnosed, procedures performed, and medications prescribed; and the ability to study a patient sample drawn from a multitude of communities and providers practicing in various settings.
In the medical literature, a considerable number of analyses have taken advantage of the longitudinal nature of claims data to identify incident case-patients with a given condition—that is, persons in whom the disease or adverse event of interest has been newly diagnosed, presumably signaling a relatively recent initial onset. Whether the researcher is seeking to examine a temporal relationship between exposures and outcomes, or the resource utilization or outcomes among persons with newly diagnosed disease, accurately distinguishing incident case-patients from nonincident case-patients (ie, those in whom the condition was pre-existing) is paramount. However, incidence estimates can be inaccurate if persons in the database who seem to have a newly diagnosed condition actually received their initial diagnosis before their enrollment in the plan.
As a way to help distinguish incident from nonincident case-patients in their analyses, researchers can incorporate a look-back period—a disease-free period leading up to the index date , when observation for the presence or absence of disease begins. Persons with a diagnosis of the condition of interest in the look-back period would then be considered nonincident case-patients. For data sets in which all beneficiaries are continuously enrolled in the medical plan for the same length of time, a look-back period from the date of entry into the medical plan until the index date could be used. However, with most claims data sets, beneficiaries enter and leave the plan at different times, and there is no consistent length of time from beneficiaries’ date of plan enrollment until the index date. By using a look-back period of a specified duration, for those who are enrolled in the plan for less than that length of time, the opportunity to have previously received a diagnostic code for the condition of interest is reduced relative to others enrolled for the entire look-back period. Such persons would thus have an increased likelihood of being misclassified as incident case-patients. An eligibility requirement of continuous enrollment in the plan for a specified duration before the index date would provide all enrollees with an equal opportunity to have previously received a diagnosis of the condition of interest.
A key question remains for researchers: How long must a disease-free look-back period be to adequately discriminate between incident and nonincident case-patients? With a longer look-back period, the likelihood of erroneously classifying patients with pre-existing disease as incident case-patients is reduced. Yet, as the look-back period increases, the pool of eligible participants decreases.
The optimal duration for a look-back period will likely vary from one condition to another. For example, persons with symptomatic or relatively serious conditions will probably be affected or otherwise concerned enough to seek frequent medical attention. For these sorts of conditions, a relatively long look-back period may be unnecessary. However, for relatively asymptomatic or less serious conditions, or for those that take longer to diagnose, a lengthier look-back period could be desirable. We explore how varying the duration of a disease-free look-back period can affect the accuracy of incident-disease classifications for 4 relatively common ocular conditions.
Methods
Data Source
The Clinformatics Data Mart database (previously named i3 InVision Data Mart) (Ingenix, Eden Prairie, Minnesota, USA) contains detailed, fully de-identified records of beneficiaries in a large nationwide managed-care network. We had data on beneficiaries receiving any eye care from January 1, 2001, through December 31, 2011. The data set contains information on beneficiaries with at least 1 International Classification of Diseases (ICD-9-CM) code for any eye-related diagnosis (360-379.9); Current Procedural Terminology (CPT-4) code for any eye-related visit or diagnostic or therapeutic procedure (65091-68899 or 92002-92499); or any claim submitted by an ophthalmologist or optometrist during the beneficiaries’ time in the medical plan. We had access to the beneficiaries’ medical claims (inpatient, outpatient, skilled nursing facility) for ocular and nonocular conditions, as well as sociodemographic information (age, sex, race, education, income). This database has previously been used in analyses involving ocular diseases. Because the data were de-identified, the University of Michigan determined that this study was exempt from requiring Institutional Review Board approval.
Eligibility
Our analysis included only persons continuously enrolled in the medical plan for the entire 11-year study period. Persons who exited and reentered the plan were excluded because we could not determine whether any eye-related diagnoses were received during their time of non-enrollment. In addition, the beneficiary must have had 1 or more visits to an eye-care provider (ophthalmologist or optometrist) during (1) the first half of 2001 (January 1 to June 30), (2) the second half of 2010 (July 1 to December 31), and (3) 2011. These time intervals are consistent with ones used in a similar analysis in which incidence overestimations for selected nonocular diseases were assessed.
Conditions of Interest
Our analysis evaluated 4 common ocular conditions: cataract, nonexudative age-related macular degeneration (ARMD), nonproliferative diabetic retinopathy (NPDR), and open-angle glaucoma (OAG). These conditions were selected because they are among the most common chronic ocular diseases affecting older Americans. Patients with these conditions were identified according to ICD-9-CM codes ( Table 1 ). The Clinformatics database captures up to 5 ICD-9-CM diagnosis codes submitted for each patient encounter. A validation study found strong agreement between ICD-9-CM codes provided by eye-care providers and the medical records for several common ocular conditions, including OAG, cataract, and retinopathy.
| Condition | Billing Codes Used |
|---|---|
| Cataract | 366, 366.0, 366.00, 366.01, 366.02, 366.03, 366.04, 366.09, 366.1, 366.10, 366.12, 366.13, 366.14, 366.15, 366.16, 366.17, 366.18, 366.19, 366.41, 366.45 |
| Nonexudative macular degeneration | 362.50, 362.51, 362.57 |
| Nonproliferative diabetic retinopathy | 362.01, 362.03, 362.04, 362.05, 362.06 |
| Open-angle glaucoma | 365.1, 365.10, 365.11, 365.12, 365.15 |
Identifying Prevalent Case-Patients
We first identified all enrollees with 1 or more codes for any of the 4 ocular conditions of interest from eye visits in the last 6 months of 2010 (July 1, 2010, through December 31, 2010). For the identified patients, we then determined whether they had another visit to an eye-care provider with a confirmatory diagnosis of the condition of interest in 2011. The rationale for requiring a visit to an eye-care provider is that these ocular conditions can be asymptomatic early in the disease course and a person may unknowingly have the condition without receiving an examination. Enrollees were considered prevalent case-patients if, according to billing codes, they had the condition of interest diagnosed in the second half of 2010 and again in 2011. Those without record of the condition during eye visits in the second half of 2010 and in 2011 were considered confirmed non-case-patients for that condition. Those who received a diagnosis in 2010 but no confirmatory diagnosis in 2011 were excluded, since we could not confirm the presence of the condition; similarly, we excluded those in whom the condition was first diagnosed in 2011.
Identifying Incident Case-Patients
We considered potential incident case-patients to be persons receiving a diagnosis of the condition of interest in the second half of 2010 and a confirmatory diagnosis in 2011. Confirmed incident case-patients were defined as the subset of these persons who had not received the diagnosis of the condition of interest in the 9.5-year look-back period from January 2001 through June 2010. These case-patients served as our gold standard, as they were known to lack the disease until the second half of 2010, when an initial diagnosis was made.
Potential incident case-patients were then confirmed or not by using look-back periods of varying lengths. Eighteen such periods were considered. The shortest period was 6 months; in each subsequent consecutive period, 6 months were added to the previous period’s duration until the longest period reached 9 years.
Determining Incidence Overestimation
For each ocular disease, we compared the incidence estimates generated by using the 18 look-back periods with our gold-standard best estimate. For each condition and look-back period, the degree of overestimation was calculated by taking the difference between the number of potential incident case-patients and the number of incident case-patients estimated by the gold standard and dividing by the number of incident case-patients. The degree of overestimation was multiplied by 100 and presented as a percentage.
Results
A total of 2457 enrollees (mean age ± standard deviation, 49.7 ± 15.1 years) met the inclusion criteria. Among the eligible enrollees, 1472 (59.9%) were female, and for those with documented information on race/ethnicity, the sample included 2010 whites (81.8%), 100 blacks (4.1%), 66 Latinos (2.7%), and 47 Asian Americans (1.9%). The sample had 793 college graduates (32.2%) and 379 persons with an annual income exceeding $125 000 (15.4%).
Open-angle Glaucoma
Among the eligible enrollees, 465 (19%) received OAG diagnostic codes at eye-care visits in the second half of 2010 and in 2011. A total of 1870 individuals (76%) had no OAG record in that 1.5-year span. The remaining 122 enrollees were excluded from this particular analysis because an OAG diagnosis was noted at least once in July through December 2010 or in 2011 but not in both periods.
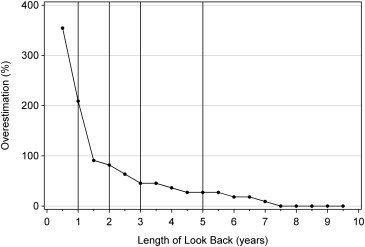
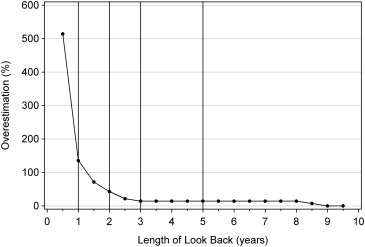
Of the 465 persons with confirmed OAG, 14 (3%) had no previous diagnosis of OAG during January 2001 through June 2010. By using a 1-year disease-free interval, OAG incidence is overestimated by 135%. With a 2-year period, overestimation drops to 43%, and with 3 years it decreases further to 14%, where it levels off for the subsequent intervals tested ( Figure 1 and Table 2 ).
| Disease-Free Interval Length | Open-angle Glaucoma | Nonexudative Macular Degeneration | Nonproliferative Diabetic Retinopathy | Cataract | ||||
|---|---|---|---|---|---|---|---|---|
| N a | Incidence Overestimation | N a | Incidence Overestimation | N a | Incidence Overestimation | N a | Incidence Overestimation | |
| 6 months | 86 | 514% | 50 | 355% | 31 | 417% | 264 | 514% |
| 12 months | 33 | 136% | 34 | 209% | 24 | 300% | 155 | 260% |
| 18 months | 24 | 71% | 21 | 91% | 19 | 217% | 107 | 149% |
| 24 months | 20 | 43% | 20 | 82% | 17 | 183% | 79 | 84% |
| 30 months | 17 | 21% | 18 | 64% | 15 | 150% | 68 | 58% |
| 36 months | 16 | 14% | 16 | 45% | 12 | 100% | 60 | 40% |
| 42 months | 16 | 14% | 16 | 45% | 12 | 100% | 56 | 30% |
| 48 months | 16 | 14% | 15 | 36% | 9 | 50% | 55 | 28% |
| 54 months | 16 | 14% | 14 | 27% | 9 | 50% | 52 | 21% |
| 60 months | 16 | 14% | 14 | 27% | 7 | 17% | 51 | 19% |
| 66 months | 16 | 14% | 14 | 27% | 7 | 17% | 50 | 16% |
| 72 months | 16 | 14% | 13 | 18% | 7 | 17% | 50 | 16% |
| 78 months | 16 | 14% | 13 | 18% | 7 | 17% | 47 | 9% |
| 84 months | 16 | 14% | 12 | 9% | 7 | 17% | 45 | 5% |
| 90 months | 16 | 14% | 11 | 0% | 7 | 17% | 44 | 2% |
| 96 months | 16 | 14% | 11 | 0% | 7 | 17% | 43 | 0% |
| 102 months | 15 | 7% | 11 | 0% | 7 | 17% | 43 | 0% |
| 108 months | 14 | 0% | 11 | 0% | 7 | 17% | 43 | 0% |
| Gold standard | 14 | 11 | 6 | 43 | ||||
a N is the number of potential incident cases. These cases were diagnosed with the disease of interest during the second half of 2010 and had a confirmatory diagnosis in 2011, and were disease free prior to that time using the disease-free intervals indicated. For example, the number of potential incident cases of open-angle glaucoma using a 6-month disease-free period is 86 enrollees. This is compared to the best incidence estimate (the Gold Standard, defined as those with a confirmed diagnosis in 2010 and 2011, along with no disease occurrence from January 1, 2001 – June 30, 2010), yielding an incidence overestimation of (86 – 14)/14 = 514%.
Among the 1870 persons with no record of OAG in the second half of 2010 and none in 2011, 157 (8.4%) had 1 or more records of OAG during eye-care visits between January 1, 2001, and June 30, 2010.
Cataract
Among the eligible enrollees, 434 persons (18%) had cataract codes in the second half of 2010 and in 2011. A total of 1625 persons (66%) had no such record in both periods. The remaining 398 enrollees were excluded from this analysis because they had a cataract diagnosis in only 1 of these 2 periods.
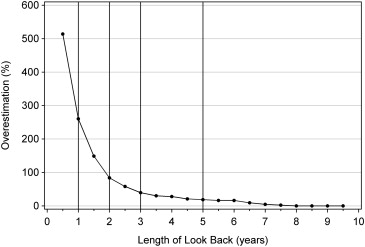
Of those with confirmed cataract, 43 (10%) had no previous cataract diagnosis during January 2001 through June 2010. Cataract incidence is overestimated by 260% with a 1-year disease-free interval, by 84% with a 2-year interval, and by 40% with a 3-year interval. With a 5-year look-back period, the incidence overestimation drops to 19%, and it decreases slowly thereafter for the subsequent periods tested ( Figure 2 and Table 2 ).
Among the 1625 persons with no record of cataract from July 2010 through December 2011, 551 enrollees (33.9%) had at least 1 previous record of the condition (ie, before July 2010). Of note, 240 of these 551 enrollees (43.6%) also had codes for pseudophakia or aphakia, which may account for their nonreceipt of a cataract code in mid-2010 through December 2011.
Nonexudative Age-Related Macular Degeneration
One-hundred three patients (4%) had codes for ARMD in the second half of 2010 and in 2011. A total of 2250 persons (92%) had no such record during eye visits in those 2 consecutive periods. The remaining persons (n = 104) were excluded from this analysis because they received an ARMD diagnosis in only 1 of these periods.
Of the 103 persons with confirmed ARMD, 11 (11%) had no record of the condition before July 2010. By using a 1-year disease-free interval, ARMD incidence is overestimated by 209%; by using 2 and 3 years, respectively, the incidence is overestimated by 82% and 45%. With a 5-year look-back period, the overestimation decreases to 27%, and it drops off slowly from there ( Figure 3 and Table 2 ).