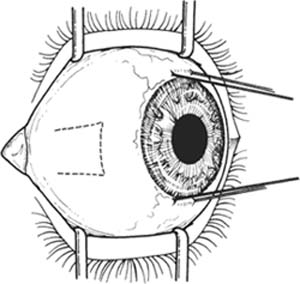
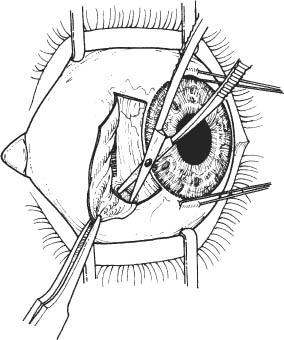
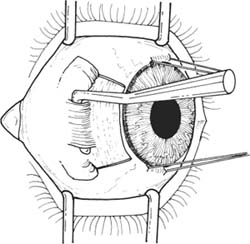
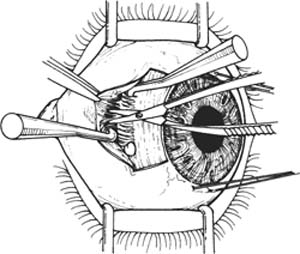
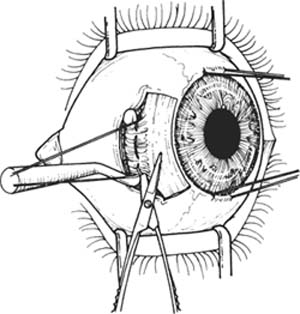
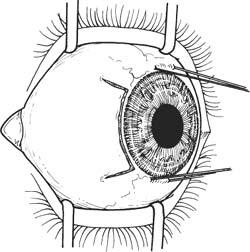
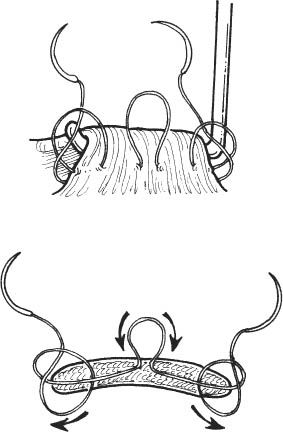
37 Extraocular muscle imbalance requiring muscle weakening for correction (e.g., medial rectus recession in esotropia). See Chapter 3. A complete strabismus evaluation with determination of the detailed surgical plan is necessary. Note: Figures are drawn from the surgeon’s viewpoint with the surgeon standing at the head of the patient. 1. Anesthesia: General anesthesia or retrobulbar/peribulbar injection plus eyelid block. 2. Place a drop of neosynephrine 2.5% into the eye to constrict the blood vessels and decrease bleeding. Prep and drape. 3. Place lid speculum. Figure 37.1 4. Place a 6–0 silk episcleral stay suture at the limbus at 6 and 12 o’clock (Fig. 37.1). Optional: Use locking Castroviejo forceps instead of stay suture. 5. Secure the globe with stay sutures to expose surgical field. Figure 37.2 6. Prepare a fornix-based, winged limbal peritomy down to bare sclera with Westcott scissors (Fig. 37.2). Figure 37.3 7. Buttonhole Tenon capsule and intermuscular septum with sharp and blunt dissection with Westcott scissors to reach bare sclera on either side of the muscle insertion (Fig. 37.3). a. Aim 45 degrees between the horizontal and vertical recti to avoid injuring the muscles. b. Bluntly spread the incision with Westcott scissors. c. Repeat on the opposite side of the muscle insertion. 8. Isolate the muscle (Fig. 37.4). a. First, sweep the Stevens tenotomy hook through the fascial buttonhole and under the muscle. Hold the hook parallel to and flush with bare sclera to facilitate passage. b. Follow with a Green muscle hook perpendicular to the sclera and just posterior to the Stevens hook. Keep the tip of the Green hook pressed against the sclera. c. Remove the Stevens tenotomy hook. Figure 37.4 d. Follow with a second Green muscle hook perpendicular to the sclera and just posterior to the first Green hook. Once again, keep the tip of the Green hook pressed against the sclera. e. Remove the first Green hook. f. The tip of the muscle hook can be visualized on the other side of the muscle. If not, repeat steps 8d–e. Figure 37.5 9. Tent the overlying conjunctiva with two Stevens tenotomy hooks and use Westcott scissors to minimally cut the check ligaments to the muscle sheath. Take care not to cut the muscle sheath or muscle or bleeding may occur. If bleeding occurs, apply direct pressure with a dental roll until it stops (Fig. 37.5). Note: Be sure to dissect the lateral rectus intermuscular septal attachments to the inferior oblique to avoid the “J Syndrome.” 10. Incise the intermuscular septum superior and inferior to the muscle minimally if necessary to obtain adequate muscle exposure. Be careful not to cut the inferior oblique muscle if incising along the inferior border of the lateral rectus. Figure 37.6 11. Suture the muscle 1 mm from its insertion with the double-armed 6–0 Vicryl with spatula needles (Fig. 37.6). a. Elevate muscle with the muscle hook. b. First throw is through half-thickness muscle from the center to one edge of the muscle, 1 mm from the insertion. Second throw is through full-thickness muscle, posterior to anterior, 1 mm from the edge of the muscle. Lock the second throw. c. Perform superiorly and inferiorly. d. Do not cut off the needles. Figure 37.7 12. Detach the muscle at its insertion with Westcott scissors (Fig. 37.7). a. Hold the muscle hook and sutures up to avoid cutting the sutures. b. Cut the muscle flush with the sclera.
Horizontal Rectus Recession
Indications
Preoperative Procedure
Instrumentation
 Lid speculum (e.g., Lancaster, Barraquer)
Lid speculum (e.g., Lancaster, Barraquer)
 Needle holder
Needle holder
 Sutures (6–0 silk with spatula needle, double-armed 6–0 Vicryl with spatula needle (S29 or S14 needle), 7–0 Vicryl suture)
Sutures (6–0 silk with spatula needle, double-armed 6–0 Vicryl with spatula needle (S29 or S14 needle), 7–0 Vicryl suture)
 Toothed forceps (e.g., Bishop-Harmon, 0.5 mm Castro-viejo)
Toothed forceps (e.g., Bishop-Harmon, 0.5 mm Castro-viejo)
 Two locking 0.5 mm toothed forceps
Two locking 0.5 mm toothed forceps
 Westcott scissors (rounded tips)
Westcott scissors (rounded tips)
 Cautery (bipolar forceps)
Cautery (bipolar forceps)
 Muscle hooks (e.g., Green, Jameson)
Muscle hooks (e.g., Green, Jameson)
 Stevens tenotomy hooks
Stevens tenotomy hooks
 Castroviejo caliper
Castroviejo caliper
Operative Procedure
Limbal Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


