(1)
Alo Eye Care, Kolkata, India
Keywords
Eyelid histologySurface epithelium tumorsTumors of the epidermisSquamous papillomaBasal cell carcinomaSquamous cell carcinomaMolluscum contagiosumChalazionAmyloidosis7.1 Eyelid Histology
Eyelid skin characteristically has no rete pegs; lanugo hairs without erector pili are present, and there is no subcutaneous fat or stratification of dermis into defined zones. The eyelid epidermis consists of four layers: the stratum corneum, stratum granulosum, stratum spinosum, and stratum germinativum. The stratum germinativum also is known as the basal layer. The dermis is composed of important structures such as hair, glands, nerves, and vessels.
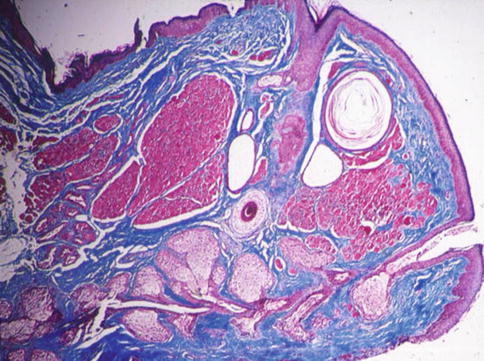
Fig. 7.1
Normal eyelid histology
7.2 Eyelid Tumors: Classification
Eyelid tumors may be classified histopathologically into the following categories for easier understanding:
(a)
Tumors of the surface epithelium
(b)
Tumors of the eyelid adnexa
(c)
Melanocytic tumors
(d)
Vascular tumors
(e)
Neurogenic tumors
(f)
Lymphocytic tumors
(g)
Tumor-like conditions
7.3 Surface Epithelium Tumors
Tumors arising from the surface epithelium may be benign, premalignant, or malignant.
7.3.1 Benign Tumors of the Epidermis
Common benign tumors arising from the eyelid epidermis include squamous papilloma, seborrheic keratosis, inverted follicular keratosis, and pseudoepitheliomatous hyperplasia.
7.3.1.1 Squamous Papilloma
Squamous papilloma is the most common benign eyelid epidermal tumor. It is characterized clinically by a wart-like lesion that may be pedunculated or sessile. Histologically, it is characterized by benign hyperplasia of squamous epithelium.
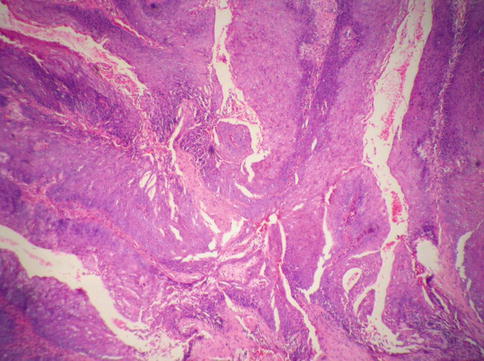
Fig. 7.2
Squamous papilloma of the eyelid
7.3.1.2 Seborrheic Keratosis
Clinically, seborrheic keratosis presents as a pigmented plaque with a stuck-on (“button-stuck”) appearance. Histologically, the epidermis shows hyperkeratosis, acanthosis, and papillomatosis, along with characteristic pseudohorn cysts.
7.3.2 Premalignant Tumors of the Epidermis
Premalignant tumors of the epidermis include keratoacanthoma, actinic keratosis, and sebaceous nevus.
7.3.2.1 Eyelid Keratoacanthoma
Eyelid keratoacanthoma typically presents with crater-like lesions and elevated margins. Clinically, it may be confused with noduloulcerative basal cell carcinoma (BCC). It is considered a variant of squamous cell carcinoma (SCC).
Histopathology
Eyelid keratoacanthoma is composed of well-differentiated squamous cells with a central keratin-containing crater.
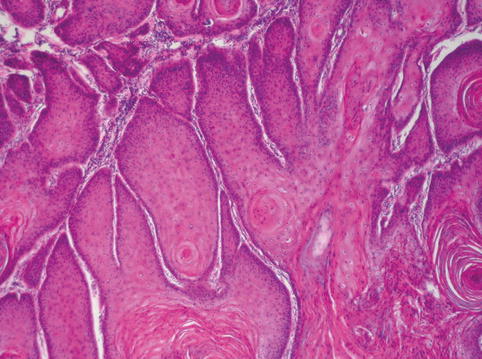
Fig. 7.3
Eyelid keratoacanthoma
7.3.2.2 Actinic Keratosis
Actinic keratosis usually presents with multiple erythematous sessile plaques that assume a horny or warty configuration.
Histopathology
The lesion is composed of acanthosis, hyperkeratosis, dyskeratosis, and atypical keratinocytes.
7.3.3 Malignant Tumors of the Epidermis
BCC (basal cell carcinoma) and SCC (squamous cell carcinoma) are the two most common malignant tumors arising from the eyelid epidermis. BCC is more common than SCC.
7.3.3.1 BCC
BCC is 39 times more common than SCC. It arises from the basal layer (stratum germinativum) of the epidermis. The most common site affected is the lower lid (65 %), followed by the medial canthus (15 %), upper lid (15 %), and lateral canthus (5 %). The clinical hallmarks of the lesion are pearly, waxy, rolled borders with telengiectasia at the borders. BCC includes the following clinical subtypes:
(a)
Nodular
(b)
Noduloulcerative
(c)
Cystic
(d)
Morpheaform or sclerosing
(e)
Pigmented
Nodular BCC is the most common clinical variety and has the best prognosis. Morpheaform BCC, the least common variant, has ill-defined margins and carries the worst prognosis. Pigmented BCC may be misdiagnosed as malignant melanoma. Although BCC does not tend to metastasize, it may affect regional lymph nodes.
Histopathology
Nodular
Nests and cords of proliferating basal cells are present.
Noduloulcerative
Peripheral palisading of tumor cells, collagen deposition in the dermis, separation of nests of tumor and dermal tumor stoma (retraction space or cracking artifacts), and central necrosis are observed.
Cystic
Cysts filled with blood and degenerated blood products, along with features of BCC, are seen.
Morpheaform
The tumor cells tend to penetrate the dermis with diffusely branching cords of cells. Peripheral palisading typically is absent.
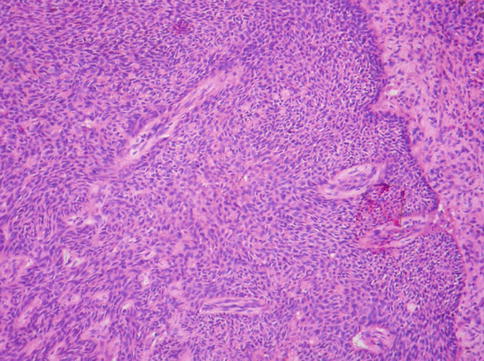
Fig. 7.4
Eyelid BCC
7.3.3.2 SCC
SCC arises from the prickle-cell layer (stratum spinosum) of the epidermis. Clinically, SCC has no pathognomonic features, and it is very difficult to differentiate it from other eyelid epidermal lesions. It may resemble BCC, sebaceous carcinoma, Merkel cell carcinoma, and benign lesions such as seborrheic keratosis. In contrast to BCC, SCC occurs more often on the upper lid. It has the potential for distant metastasis.
Histopathology
SCC progresses through three phases:
(a)




Intraepithelial squamous dysplasia: partial thickness of epithelium by dysplastic cells
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
