Purpose
To investigate the ocular and neurologic manifestations, and to identify the causative mutation in a family with an excavated optic disc anomaly, high myopia, enlarged axial lengths, and abnormal visual evoked response (VER).
Design
Prospective observational case series with whole exome sequencing.
Methods
Institutional study of 8 family members from 3 generations. Clinical examination included visual field examination, optical coherence tomography, axial length measurement, audiometry, visual evoked response (VER), orbital and cerebral magnetic resonance imaging (MRI), and renal ultrasound. DNA was analyzed by whole exome sequencing and Sanger sequencing. Main outcome measures were clinical and radiological findings, and DNA sequence data.
Results
Three affected family members, a father and his 2 daughters, were examined. The parents and siblings of the father were healthy. Affected individuals presented with excavated optic discs, high myopia (−1.00 to −16.00 diopters), and increased axial lengths. Reduced visual acuity (0.05–0.8) and decreased sensitivity on visual field examination were observed. VER revealed prolonged latency times. Affected eyes appeared ovoid on MRI and the father had thin optic nerves. Exome sequencing revealed that the father was heterozygous for a de novo 5 bp deletion in MYCBP2 , c.5906_5910del; p.Glu1969Valfs*26. The same mutation was found in his 2 affected daughters, but not in his parents or siblings, or in public databases.
Conclusion
We describe a distinct excavated optic disc anomaly associated with high myopia and increased axial length. The condition appears to follow an autosomal dominant pattern and segregate with a deletion in MYCBP2 . We suggest naming this entity high myopia–excavated optic disc anomaly.
Excavated optic disc anomalies traditionally include optic disc coloboma, morning glory disc anomaly, peripapillary staphyloma, optic pit, and megalopapilla. Recently, 2 more distinct variants have been recognized, 1 associated with periventricular leukomalacia and the other the vacant optic disc seen in papillorenal syndrome (MIM #120330).
Correct classification of congenital optic nerve malformations can be difficult, as the clinical features often overlap. It is, however, important to ensure prompt diagnosis of their specific associated systemic findings, exemplified by the central nervous system and endocrinologic disturbances associated with optic nerve hypoplasia and the renal abnormalities associated with vacant disc anomalies.
In the present work, we examined a family in which the father and his 2 daughters presented with a unique excavated optic disc anomaly. In addition to optic nerve dysplasia, high myopia, enlarged axial lengths, and abnormal visual evoked response (VER) were found. The parents and the siblings of the father were healthy. Trio exome sequencing of the affected father and his parents revealed 2 de novo mutations in the father. Only 1 of these, a 5 bp frameshift deletion in MYCBP2 (MIM*610392), was present in all affected individuals. MYCBP2 is a large multifunctional protein that has been shown in experimental animals to be important for axonal outgrowth and guidance in the development of the visual pathways.
Methods
Family Study
This is a prospective observational case series and a genetic laboratory investigation that included review of medical records; clinical, electrophysiological, and radiological examination; and whole exome sequencing. Patients and their unaffected family members were invited to participate in the study. The purpose and the procedure of the study were explained to all participants and all signed an informed letter of consent. Parental consent was obtained for the 12-year-old girl included. The study adhered to the tenets of the Declaration of Helsinki, and the study as well as the letter of consent were approved by the Regional Committee for Medical and Research Ethics, Western Norway (Institutional Review Board [IRB] no. 00001872, ref. no. 2012/329). Approval included permission to obtain data from medical records and to perform clinical and radiological examinations, and genetic analysis.
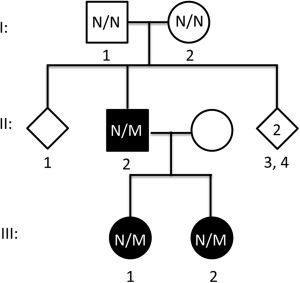
The family pedigree is shown in Figure 1 . The unaffected parents of the proband (I-1 and I-2) and his siblings underwent a routine ophthalmologic examination while affected family members underwent an extended clinical examination including measurements of visual acuity (Snellen chart), intraocular pressure (IOP) (Goldmann tonometry), axial length (Zeiss IOL Master 500; Carl Zeiss Meditec, Jena, Germany), stereopsis (Lang stereotest, Titmus stereotest), retinal correspondence (Bagolini striated lens test), color vision (Ishihara and Farnsworth D15 color vision tests), and visual field (Octopus 900 perimeter program G2 dyn; Haag-Streit Diagnostics, Koenitz, Switzerland). Fundus photographs and spectral-domain optical coherence tomography (OCT) (Topcon 3D OCT-1000 Mark II; Topcon Corporation, Tokyo, Japan) of the macula and optic disc were obtained. In addition, a detailed neurologic examination was performed. All affected family members underwent cerebral and ocular 3 Tesla magnetic resonance imaging (MRI), testing of VER, pure tone and speech audiometry, and renal ultrasound examination.
Isolation of DNA, Genotyping, and Exome Sequencing
Blood samples for genotyping were obtained from all family members. Genomic DNA was isolated from blood. Targeted capture and trio exome sequencing were performed at HudsonAlpha Institute for Biotechnology (Huntsville, Alabama, USA). Exome capture was performed using Roche-NimbleGen Sequence Capture EZ Exome v2 kit and paired-end 100nt sequencing on the Illumina HiSeq. The paired-end reads were aligned to the hg19 reference genome using the Burrows-Wheeler Alignment tool (BWA v.0.5.8c), providing between 6.1 and 14.4 gigabases of aligned sequence data for the 3 samples. This resulted in an average of 56X median coverage of the target capture regions with 96% of target bases covered at least 8X. After the alignment, PCR duplicates were removed with Picard v1.90 ( http://broadinstitute.github.io/picard ), and Genome Analysis Toolkit (GATK nightly-2013-07-09-gce5e621) was used for base quality recalibration, realignment around known indels, and multisample variant calling (GATK’s UnifiedGenotyper tool) according to GATK’s Best Practices workflow. Minimum depth of coverage required to consider a variant was set to 8X for total depth and 5X for the variant allele. ANNOVAR was used for variant annotation. Coding and putative splice sites (defined as 2 bps flanking coding exons) were filtered against variants with MAF frequency >0.8% in an in-house database of more than 300 Norwegian exomes and variants present at >0.5% allele frequency in the 1000 Genomes database (phase 1 release v3 called from 20101123 alignment). The de novo mutations were verified by Sanger sequencing. The entire coding region of PAX2 was Sanger sequenced in the proband.
RNA Analysis
Total RNA was purified from blood using the Tempus system (Life Technologies, Carlsbad, California, USA). Reverse transcription and cDNA synthesis were performed using the SuperScript VILO cDNA synthesis kit (Life Technologies). The expression of wild-type and mutant MYCBP2 was detected by Sanger sequencing using primers spanning exon junctions near the mutation of interest.
Results
Ophthalmologic Examination
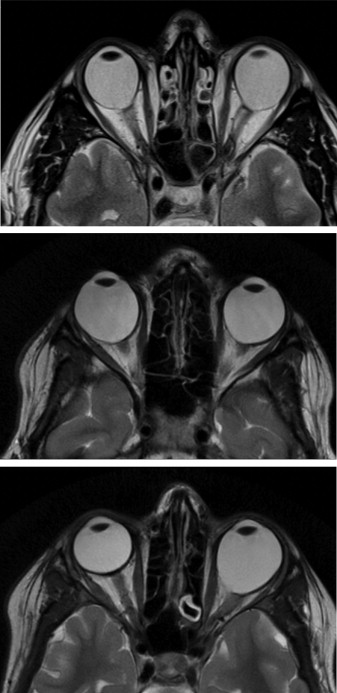
The ocular findings are illustrated in Figure 2 and the Supplemental Figure (available at AJO.com ), and the MRI findings are shown in Figure 3 . The clinical findings are summarized in the Table .
| Patient | |||
|---|---|---|---|
| II-2 | III-1 | III-2 | |
| Pregnancy and birth | 10 days post-term | Maternal bleeding, otherwise normal | Maternal bleeding, otherwise normal |
| Presenting symptom | Strabismus | Reduced vision | None (detected at routine examination at 4 years) |
| Subjective progression | No | No | No |
| General development | Normal | Normal | Normal |
| Dysmorphic features | None | None | None |
| Height (mid-parental height) (cm) | 167 (163.5), 2.5nd percentile | 157 (168.5), 10th percentile | 140 (168.5), 3rd percentile |
| Urine test strip, serum electrolytes, creatinine, urea | Normal | Normal | Normal |
| Renal ultrasound | Several small hyperechoic foci near the apex of the papillae of the pyramids | 1–3 small hyperechoic foci near the papillary apex | Normal |
| Strabismus | Exophoria | Exophoria | Left hypotropia |
| Patching | Yes | No | Yes |
| Motility | Normal | Normal | Nd |
| Convergence | Reduced | Reduced | Nd |
| Stereopsis/retinal correspondence | None detectable | Titmus stereo test positive | None detectable |
| Horizontal corneal diameter (mm) | 11/11.5 | 11.5/11.5 | 11.5/11.5 |
| Central corneal thickness | Nd | Nd | 568/566 μm |
| Anterior segment | Normal | Normal | Normal |
| Optic disc | Dysmorphic | Dysmorphic | Dysmorphic |
| Retina | Choroidal nevus OD | ||
| Axial length (mm) | 27.11/28.99 | 29.27/27.27 | 23.4/29.03 |
| Refraction (D) | −10.00 −2.50 × 20/−14.00 −1.50 × 180 | −16.00 −1.50 × 170/−11.50 −1.75 × 170 | −1.00 −0.50 × 180/−15.75 −3.50 × 180 |
| Best-corrected visual acuity | 0.32/0.63 | 0.32/0.4 | 0.8/0.05 |
| Intraocular pressure (mm Hg) | 14/13 | 16/16 | 17/18 |
| Color vision | Red-green defect | Normal | Normal |
| P100 (ms) | 118.2/121.5 | 116.4/116.4 | 103.5/Nd |
The proband (Patient II-2), aged 47 years, is the second child of unrelated, healthy parents and has 3 unaffected siblings. There was no history of similar congenital eye disease in the family. An intermittent convergent squint was noted at the age of 6 months. At age 18 months he was examined by an ophthalmologist, who noted bilateral anomalies of the optic discs interpreted as optic disc coloboma. The anterior segment and the intraocular pressure were normal in both eyes (OU). The earliest refraction reported in his medical journal was at the age of 4 years (−4.50/−6.00, OD/OS respectively). His best-corrected visual acuity (BCVA) at the age of 8 years was 6/18 and 6/9 (Østerberg chart). The refraction remained stable in childhood but later the myopia gradually increased.
When examined for this study, his BCVA was −10.00, −2.50 × 20: 0.32 (OD) and −14.00, −1.50 × 180: 0.63 (OS). The axial lengths were 27.11 mm (OD) and 28.99 mm (OS). Ophthalmoscopy revealed grossly dysplastic optic discs that were deeply excavated on OCT ( Figure 2 ). Pigmentary changes involving the macular region were present ( Supplemental Figure , available at AJO.com ). A general reduction of sensitivity was found on visual field examination, most pronounced in his right eye ( Figure 2 ). There was a moderate red-green color vision defect. VER showed reproducible and clear waveforms with pathologically prolonged latencies bilaterally. On MRI both eyes appeared ovoid and both optic nerves were thin. The optic chiasm was normal ( Figure 3 ).
Patient III-1 is the 16-year-old daughter of Patient II-2. She presented with reduced visual function aged 2 years. At the age of 5, she was found to be myopic, −6.00, −2.00 × 160 (OD) and −3.50 (OS). BCVA was 4/6- (OU). When examined for this study, her BCVA was −16.00, −1.50 × 170: 0.32 (OD) and −11.50, −1.75 × 170: 0.4 (OS). Her axial lengths were 29.27 mm (OD) and 27.27 mm (OS). Dysplastic optic discs that were deeply excavated on OCT were found. There was a general reduction of sensitivity on visual field examination ( Figure 2 ). Color vision was normal. Prolonged latencies were found on VER but were less pronounced than in the proband. Both eyes were ovoid on MRI while the optic nerves, chiasm, and the brain were normal ( Figure 3 ).
Patient III-2 is the 12-year-old daughter of Patient II-2. At the age of 4 she was found to be highly anisometropic (+1.00/−10.00 OD/OS, respectively) with reduced visual function in her left eye. When examined for this study, BCVA was −1.00, −0.50 × 180: 0.8 (OD) and −15.75, −3.50 × 180: 0.05 (OS). Axial lengths were 23.42 mm (OD) and 28.38 mm (OS). Ophthalmoscopy revealed a grossly dysplastic left optic disc with less pronounced changes in the right eye. Here the presence of a central excavation and no central retinal circulation suggested a vacant disc. A general reduction of sensitivity was found in the left eye on visual field examination and a scotoma in the lower temporal quadrant was present in the right eye ( Figure 2 ). Color vision was normal. VER was normal on her right side, but on the left side the examination was suboptimal and difficult to interpret. On MRI, her left eye was ovoid while the right eye appeared normal. The optic nerves, chiasm, and the brain were normal ( Figure 3 ).
General Examination
Apart from the visual disturbances, all patients were healthy, of normal intelligence, and with no dysmorphic features. There were no symptoms or signs of connective tissue involvement like joint hyperextensibility or heart valve abnormalities. Neurologic examination, including assessment of the olfactory nerve, was entirely normal. Audiograms were within the normal range, but in Patient II-2 a shallow depression in the midrange could be consistent with a mild form of hereditary hearing loss. Speech perception was normal in all patients. Patients II-2 and III-1 had small hyperechoic foci near the apex of the papillae of the renal pyramids interpreted to be a normal variant. There were no clinical or biological signs of renal disease. All patients had a stature in the lower normal rank; II-2 was 167 cm (2.5nd percentile), III-1 was 157 cm (10th percentile), and III-2 was 140 cm (3rd percentile). Mid-parental height of the parents of the proband was 163.5 cm.
Genotyping/Exome Sequencing
We performed whole exome sequencing of the proband (II-2) and his parents (I-1, I-2), searching for a de novo mutation. We found 18 263 exonic variants in the proband. Variant filtration against noncoding and common variants yielded 245 rare coding variants that were compared against whole exome data from his parents. This analysis revealed only 2 true de novo mutations, a 5 bp deletion in MYCBP2 (c.5906_5910del; p.Glu1969Valfs*26, NM_015057.4) and a synonymous mutation located 2 bp before an exon-intron boundary in PDCD6 (c.C366T (p.=)). Although our in silico analysis did not suggest that the latter mutation would influence normal splicing, we performed Sanger sequencing of both mutations in the pedigree and only the MYCBP2 frameshift deletion was present in both the proband and his affected children and absent in his parents and siblings. Sanger sequencing of cDNA from peripheral blood mRNA from 2 affected individuals confirmed the presence of the MYCBP2 c.5906_5910del mutation in the expected 50% ratio. The variant is located in exon 40 of the gene and has not been reported in publically available databases including the 1000 Genomes database and dbSNP. Furthermore, the mutation has not been seen in our own in-house database of variants from more than 300 whole exomes of Norwegian individuals.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


