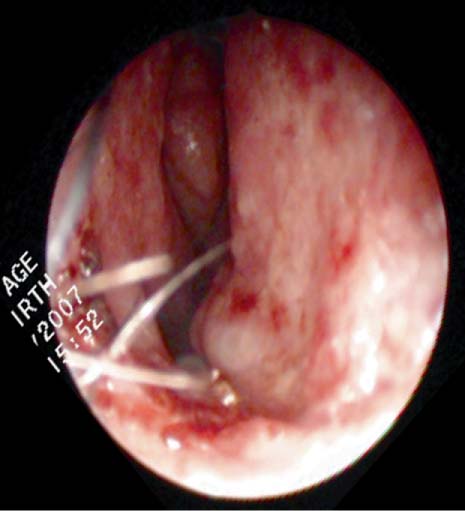
45 A 19-year-old man with a history of nose-bleeds that are increasing in frequency and becoming harder to control recently required an anterior nasal pack to control bleeding. This patient reports no nosebleeds before age 15, no history of nasal trauma, no history of sinusitis or recurrent upper respiratory tract infections, and no history of prolonged bleeding associated with cuts or bruising. The nosebleeds seem to begin spontaneously. Ordinarily he has no complaints of nasal obstruction except that the bleeding has caused some persistent nasal crusting. The patient notes that his father had recurrent nosebleeds over the years, requiring frequent nasal packing and even blood transfusions on occasion, but had died unexpectedly from a stroke several years earlier. His mother reports no history of nosebleeds. The patient has an older brother and younger sister, both without a history of nosebleeds. On physical examination the patient is a well-appearing man with no signs of bruising. On head and neck examination, a small hyper-emic blemish is noted on his lower lip (Fig. 45.1) and conjunctivae. Nasal endoscopy is performed and demonstrates these same blemishes along his nasal septum with residual crusting from his previous bleed and a small telangiectasia on the right inferior turbinate (Figs. 45.2 and 45.3). Fig. 45.1 Telangiectasia noted on lower lip suggestive for hereditary hemorrhagic telangiectasia. Fig. 45.2 Multiple telangiectasias noted on the right anterior nasal septum. 1. The differential diagnosis for nasal bleeding is large. A. In young children nasal trauma predominates and usually occurs on the side of their dominant hand. Other sources of mucosal irritation can also predispose to bleeding, including inflammation from infection, drying of the nasal mucosa, foreign bodies, and allergic rhinitis. The Kiesselbach plexus on the anterior septum is the region most likely to bleed with nasal trauma. Fig. 45.3 Small telangiectasia on the inferior aspect of right inferior turbinate. B. Granulomatous diseases, including Wegener and syphilis, can cause bleeding. C. Hypertension often associated with renal disease and aortic coarctation can be a cause. D. A large array of coagulapathies, including von Willebrand disease and the hemophilias, are relatively common and cause variable bleeding presentations that may include the nose. E. Although rare, vitamin C deficiency with scurvy causes nasal bleeding as well as bleeding from other sites. F. Any nasal mass can cause epistaxis, whether it is inflammatory or neoplastic. Be particularly wary with juvenile nasopharyngeal angiofibroma in the setting of unilateral nasal obstruction and epistaxis in an adolescent male. G. An array of vascular malformations, including hereditary hemorrhagic telangiectasia (HHT), can be the cause of recurrent bleeding. 2. HHT, also known as Osler-Weber-Rendu syndrome, has dilated subepithelial vessels as the hallmark of the disease. Multiple arteriovenous malformations (AVMs) are present that lack intervening capillaries, resulting in direct connections between arteries and veins. These AVMs lack the usual contractile elements and therefore tend to bleed easily and profusely. 3. Small AVMs are referred to as telangiectasias
Hereditary Hemorrhagic Telangiectasia
History

Differential Diagnosis—Key Points

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


