Surgery with transoral robotic surgery (TORS) offers significant advantages compared with traditional open surgical approaches and potentially minimizes the long-term side effects of organ preservation therapy with chemoradiation. Angled telescopes and wristed instruments allow visualization and access to areas of the pharynx that are difficult to reach with line-of-sight instrumentation. Although the application of TORS in head and neck surgery has expanded considerably, there are still only limited data available on the postoperative complications and their management. As further data become available, it is likely that further risk factors and treatment strategies will become available.
Key learning points
At the end of this article, the reader will:
- •
Know the vascular anatomy that is relevant to transoral robotic surgery (TORS).
- •
Know the techniques for intraoperative hemostasis during TORS.
- •
Know the risk factors for postoperative hemorrhage following TORS.
- •
Know the techniques for gaining hemostasis in secondary hemorrhage following TORS.
Introduction
Transoral robotic surgery (TORS) is an emerging technique in the management of both benign and malignant neoplasms of the head and neck. Following the first feasibility study by Hockstein and colleagues in 2005 and subsequent approval from the US Food and Drug Administration (FDA) in 2009, the use of this minimally invasive technology for resection of lesions of the upper aerodigestive tract has flourished. There is a growing body of literature to support the functional and oncologic outcomes of TORS in malignant lesions of the oropharynx, hypopharynx, supraglottis, and glottis and also for its use in resection of benign tongue base conditions such as obstructive sleep apnea. It is likely that the applications for TORS in the head and neck will continue to grow and be further refined with increasing experience.
Compared with traditional open surgical techniques, robotic surgery has a different anatomic perspective. Transoral surgeons approach the anatomy from the inside out and this change in perspective can initially be disorientating, potentially increasing the complications of surgery. One such complication is bleeding from major branches of the external carotid artery. When considering hemostasis in TORS it is essential to have an adequate understanding of this different anatomic perspective in order to minimize complications.
Introduction
Transoral robotic surgery (TORS) is an emerging technique in the management of both benign and malignant neoplasms of the head and neck. Following the first feasibility study by Hockstein and colleagues in 2005 and subsequent approval from the US Food and Drug Administration (FDA) in 2009, the use of this minimally invasive technology for resection of lesions of the upper aerodigestive tract has flourished. There is a growing body of literature to support the functional and oncologic outcomes of TORS in malignant lesions of the oropharynx, hypopharynx, supraglottis, and glottis and also for its use in resection of benign tongue base conditions such as obstructive sleep apnea. It is likely that the applications for TORS in the head and neck will continue to grow and be further refined with increasing experience.
Compared with traditional open surgical techniques, robotic surgery has a different anatomic perspective. Transoral surgeons approach the anatomy from the inside out and this change in perspective can initially be disorientating, potentially increasing the complications of surgery. One such complication is bleeding from major branches of the external carotid artery. When considering hemostasis in TORS it is essential to have an adequate understanding of this different anatomic perspective in order to minimize complications.
Relevant anatomy
- •
It is important to have an understanding of the inside-out anatomy, which is significantly different from the anatomy of an open approach
- •
The parapharyngeal fat is an important landmark for the internal carotid artery
- •
The styloid muscular diaphragm is a guide to the vasculature because the major vessels lie lateral to this
The oropharynx extends from the superior surface of the soft palate to the superior surface of the hyoid bone. It is composed of the soft palate and the uvula, anterior and posterior tonsillar pillars, palatine tonsils, glossotonsillar sulci, base of tongue, and the posterior and lateral pharyngeal walls. There is a rich vascular supply to this region from the external carotid artery with multiple anastomoses between various branches of this major arterial system. An understanding of the vascular anatomy and the relation of this to the surrounding muscular anatomy is important for minimizing the risk of significant bleeding during TORS surgery ( Fig. 1 ).
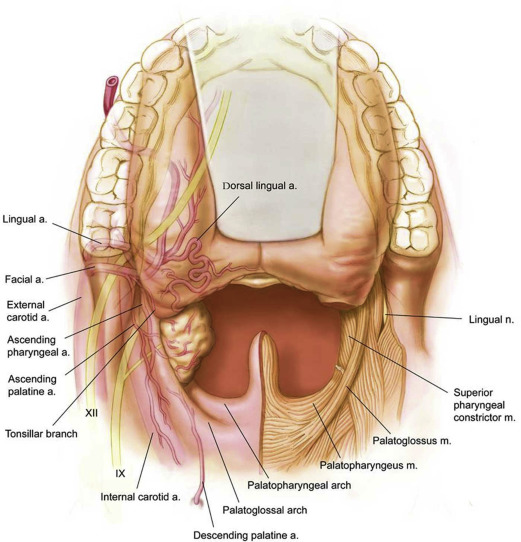
The first muscular landmark of importance is the superior pharyngeal constrictor muscle with the underlying buccopharyngeal fascia. Deep to this buccopharyngeal fascia lies the medial pterygoid superiorly and parapharyngeal space more inferiorly. The internal carotid artery is protected in the region of the parapharyngeal space only by a layer of parapharyngeal fat and pulsations can often be appreciated in this region. Surgeons should avoid dissecting lateral to the pharyngeal fat pad so as not to encounter the internal carotid artery and so that this fat provides protection to the carotid arterial system postoperatively.
The next important landmarks are the stylopharyngeus and styloglossus; these form the styloid diaphragm and most vascular structures lie lateral to these muscles. The stylopharyngeus muscle spans from the base of the styloid process lateral to the superior constrictor before passing between the superior and middle constrictor muscles to attach onto the posterior border of the thyroid cartilage and the palatopharyngeus muscle. The styloglossus muscle is positioned more superficially and laterally to the stylopharyngeus and arises from the inferior and lateral edge of the styloid process, broadening out as it descends to insert into the lateral aspect of the tongue. Following identification of these muscles, surgeons typically encounter the tonsillar branch of the glossopharyngeal nerve, which often courses between these two muscles.
Vascular Supply of the Tonsillar Fossa
The tonsillar fossa receives supply from the:
- •
Lingual artery
- ○
Tonsillar branch of dorsal lingual artery
- ○
- •
Facial artery
- ○
Tonsillar branch
- ○
Ascending palatine branch
- ○
- •
Ascending pharyngeal artery
- •
Internal maxillary artery
The blood supply of the tonsillar fossa comprises the tonsillar branch of the dorsal lingual artery, tonsillar and ascending palatine branches of the facial artery, ascending pharyngeal artery, and internal maxillary artery ( Fig. 2 ).
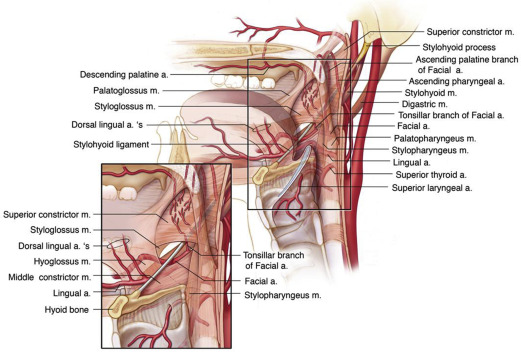
The tonsillar branch of the dorsal lingual artery approaches from inferolateral to the tonsil to pierce the superior constrictor muscle laterally and provide the main blood supply to the tonsillar fossa. The ascending palatine branch of the lingual artery arises close to the origin of the facial artery and ascends between the styloglossus and stylopharyngeus. The tonsillar branch of the ascending palatine artery pierces the superior constrictor muscle to supply the fossa.
The ascending pharyngeal artery divides into pharyngeal and neuromeningeal branches. The pharyngeal branch divides into superior, middle, and inferior pharyngeal arteries and the middle and inferior branches supply the tonsillar fossa.
The internal maxillary artery supply is from the descending palatine artery, which travels through the lesser palatine canal to reach the tonsillar fossa and anastomose with the ascending palatine.
Vascular Supply of the Base of Tongue
The pharyngeal part of the tongue is covered by lymphoid tonsillar tissue that is contiguous with the palatine tonsil at the glossotonsillar sulcus. Immediately deep to this tissue lies the intrinsic tongue musculature.
The main issue when considering the vasculature of the base of tongue is to understand the course of the lingual artery and its branches. It arises from the external carotid artery at the level of the hyoid bone and continues lateral to the middle constrictor muscle until the hypoglossal nerve crosses it. From here it passes deep to the hyoglossus muscle and runs along the superior surface of the hyoid bone. It is in this position that it is most likely to be encountered during TORS. Here it divides into 4 branches, with the most important branch for consideration in TORS being the dorsal lingual artery, which supplies the base of tongue.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


